Case 5 Index
Introduction
ED Bounceback
Outcome
Nurse Depositions
Nurse Expert Witnesses
Physician Depositions
Physician Expert Witnesses
Legal Outcome
Documentation Review
Medical Review
The decision to not obtain a head CT is the primary issue to consider in this case. There are numerous recommendations and guidelines that help ED physicians make appropriate imaging decisions after head trauma. The patient was anticoagulated (initially with a subtherapeutic INR and then with enoxaparin as well as a dose of warfarin), fell, and had visible head trauma. He was acting normally, without any significant deficit in GCS or abnormality on neurologic exam.
The most popular and well-researched guideline for imaging in the ED after head trauma is the Canadian CT Head Injury Rule. This patient unfortunately does not meet criteria for application of this rule, due to being anticoagulated. Additionally, he does not qualify for this rule because he did not lose consciousness, did not have amnesia to the event, and was not disoriented.

Generally speaking, patients who meet criteria for exclusion from Canadian Head CT Rule undergo a CT scan, with the exception of pediatric patients, for which the PECARN rule is used.
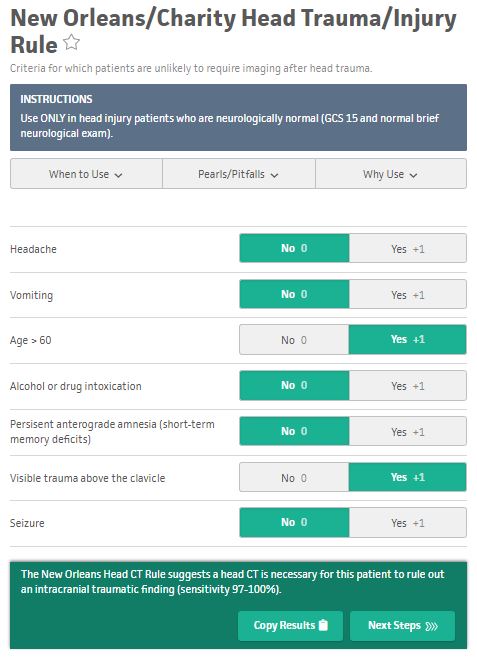
Another clinical decision rule that is less popular is the New Orleans Head Trauma Rule. The patient would qualify for application of this rule. Based on his age and the fact that he has visible trauma above the clavicle, this rule suggests that a head CT is necessary.
Finally, the ACEP clinical policy makes a level B recommendation that a head CT “should be considered in head trauma patients with no loss of consciousness or posttraumatic amnesia” if the patient meets a number of criteria, one of which is a coagulopathy. The wording of this policy only suggests that a CT scan should be considered, which is unfortunately not helpful. (Source)
One of the key issues seems to be the patient’s anticoagulation status. He had an INR done that was subtherapeutic. The physician mentions this in his note, and seems to use this as part of his rationale for not obtaining a head CT. Even though the patient was subtherapeutic, his INR was still elevated, placing him at increased risk for bleeding. Furthermore, the patient had received a dose of warfarin and a dose of enoxaparin after his INR was tested. The subtherapeutic INR was unfortunately not reflective of the patient’s true state of anticoagulation. It seems that outdated and incorrect information was used to make the decision to not obtain a head CT.

Another important issue is the importance of handoffs and how to document them. The patient’s care was transferred between 2 physicians, and there was a flaw in the 2nd physician’s understanding of a critical piece of information. We do not know if this flaw was due to a poor handoff. Documenting that a handoff occurred is important, but it is unreasonable to document every detail of that discussion. The accepted standard is to document who took over the patient’s care, and a very brief explanation of the plan. Remember that the point of communicating information during a handoff is to help the receiving physician understand the situation, not to enable to the outgoing doctor to engage in “I told you so” documentation. Furthermore, the outgoing physician is not responsible for predicting unexpected and rare future events, as occurred in this case.
Another element of consideration is the initial physician’s plan to admit the patient. She made this decision after obtaining most of his test results, with the exception of his DVT ultrasound. It is difficult to appreciate any objective indication for admission from any of his testing. There is no clear explanation for why the patient would need to be admitted, especially if the DVT ultrasound was negative. In hindsight, admitting the patient would have avoided the tragic outcome, but there was no way to know this prospectively. This premature decision to admit the patient seems inappropriate with the information given.
There is some interesting research about EM medical malpractice and the use of clinical decision rules for in head trauma. Lindor et al reviewed 48 medical malpractice lawsuits regarding patients with head injuries and the decision to obtain CT scans. The physician was found negligent in 10 lawsuits, not liable in 27 lawsuits, and settled in 11 lawsuits. In the 10 cases where the physician was found to be negligent, every clinical decision rule would have indicated the need for head CT. (Source)
A final element of this case is the fact that the patient wanted to leave the ED after hitting his head. This fact is referenced in the physican’s note. Unfortunately, discharging a patient because they want to leave the ED is very different from recommending a test and having them sign out AMA. There is little room for shared decision-making when the correct clinical course is unambiguous. The patient had been in the ED all day, and then rapidly returned. The patient clearly did not want to be there any longer, and it is understandably frustrating for the physician to work hard to take care of the patient for hours, discharge the patient, and then have him come right back. The cognitive inertia towards discharge likely played a role in both parties wanting to avoid further time-consuming testing.
There were many factors that played into this bad outcome. These factors include a handoff between 2 doctors, a misunderstanding of the patient’s state of anticoagulation, a missed opportunity to order a head CT, and cognitive inertia leading toward discharge on the part of both the doctor and the patient. The patient’s death is a tragic outcome, and reviewing this case can help avoid similar situations in the future.