Welcome to medmalreviewer.com! The purpose of this site is to improve doctor’s medical knowledge and documentation by reviewing real-life malpractice cases. These cases are presented in long form, deep dive fashion, published monthly. Each case is broken down into several posts. To see more info about the website, here are links to the About Page and FAQs. Another helpful overview post is the 3 Goals of Documentation. I’ve created a Documentation Template to help doctors write notes that are easy to defend, and a Documentation Rubric to grade notes from malpractice cases.
Special thanks to Jeremy Faust (@jeremyfaust) for peer review of this month’s case.
Home Page
Case 1: Shortness of Breath
Case 2: Fever
Case 3
Introduction
Outcome
Deposition
Legal
Documentation
Medical Review
This case is about a 17-year-old young woman who was using heroin one evening with a friend. She became unresponsive, stopped breathing, and the friend called 911. Her friend attempted to help her by putting her in an ice cold bath and doing chest compressions. As seen below, EMS is called and the patient is found lying in the doorway of the bathroom, unresponsive and apneic, but with a carotid pulse.

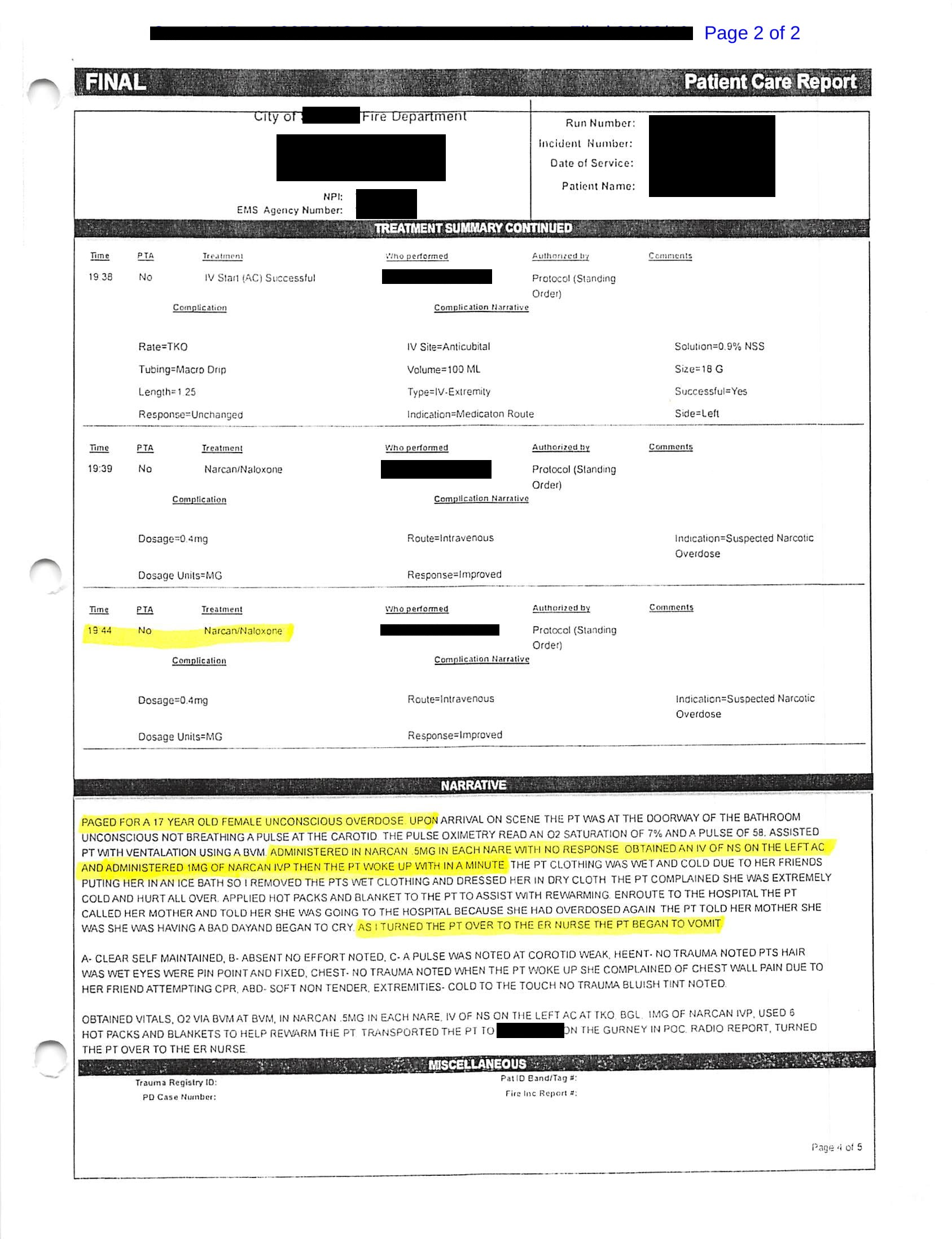
The narrative section of the note gives a description of her ABCs: airway is clear, she was making no respiratory effort, weak carotid pulse, wet hair and pupils that are pinpoint and fixed. Documentation of initial oxygen saturation is listed at 7% and heart rate of 58. EMS immediately began to bag the patient with a BVM. The narrative section of the run report lists an attempt of 0.5mg Narcan in each nare, although this conflicts with the treatment section above it. It seems the patient had no response, therefore 18g IV access was obtained in her left antecubital fossa. Narrative states that the patient was then given 1mg naloxone via IV. Medication log above lists two 0.4mg Narcan doses given via intranasal route. The patient then woke up “within a minute”.
After wakening, EMS then removes her wet and cold clothing and attempts to warm her up with hot packs and a blanket. The patient was coherent enough to call her mother to inform that she overdosed and was going to the hospital. She reports to EMS that she is cold and that her chest hurts due to her friend attempting CPR. On arrival to the ED, her care is handed over to the ER nurse.
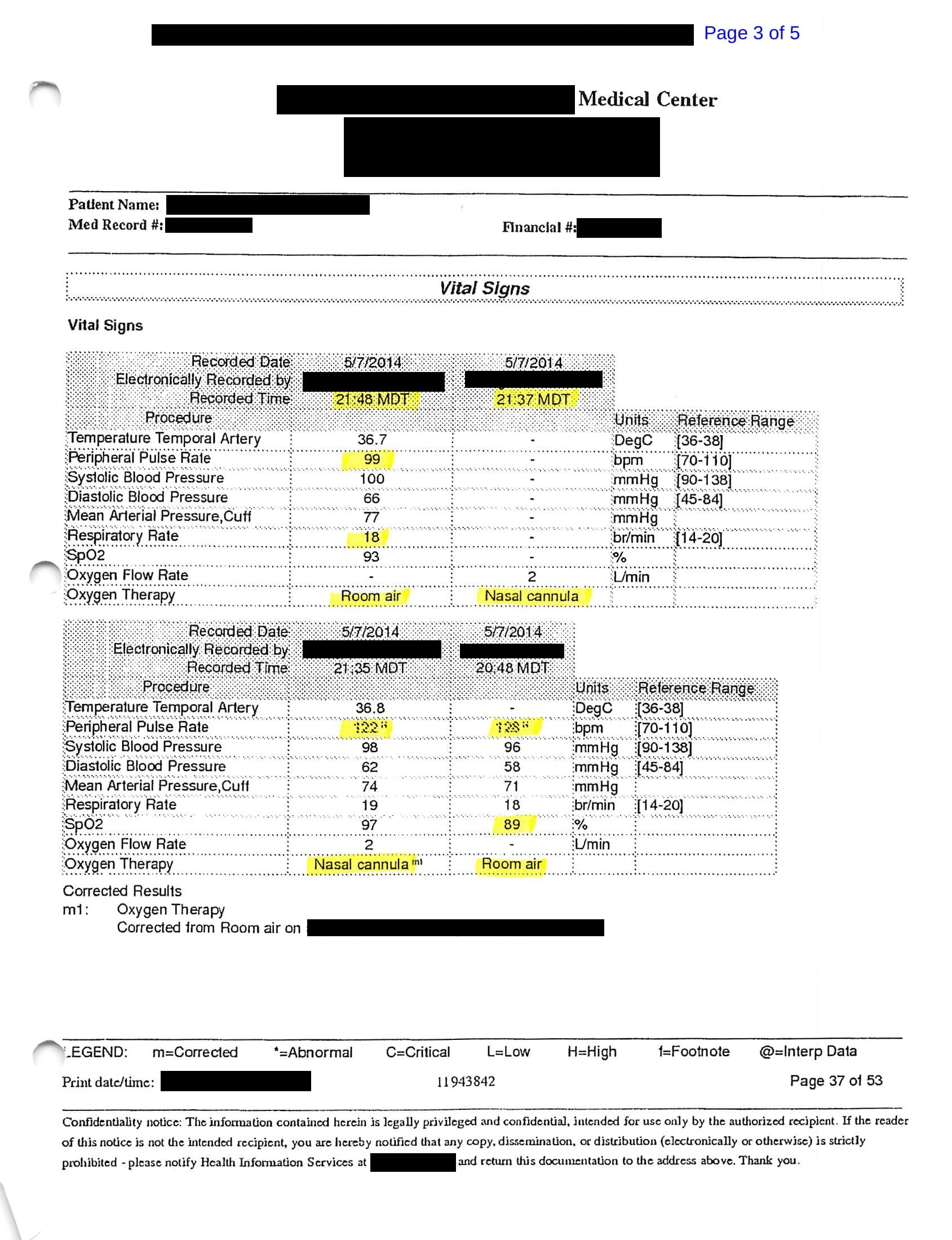
Vital signs are shown below, displayed in reverse chronological order.
The physician documents that he saw the patient at 8:40pm, which is immediately at her arrival time. This ED documents on T-sheets, and the medical record is shown here:
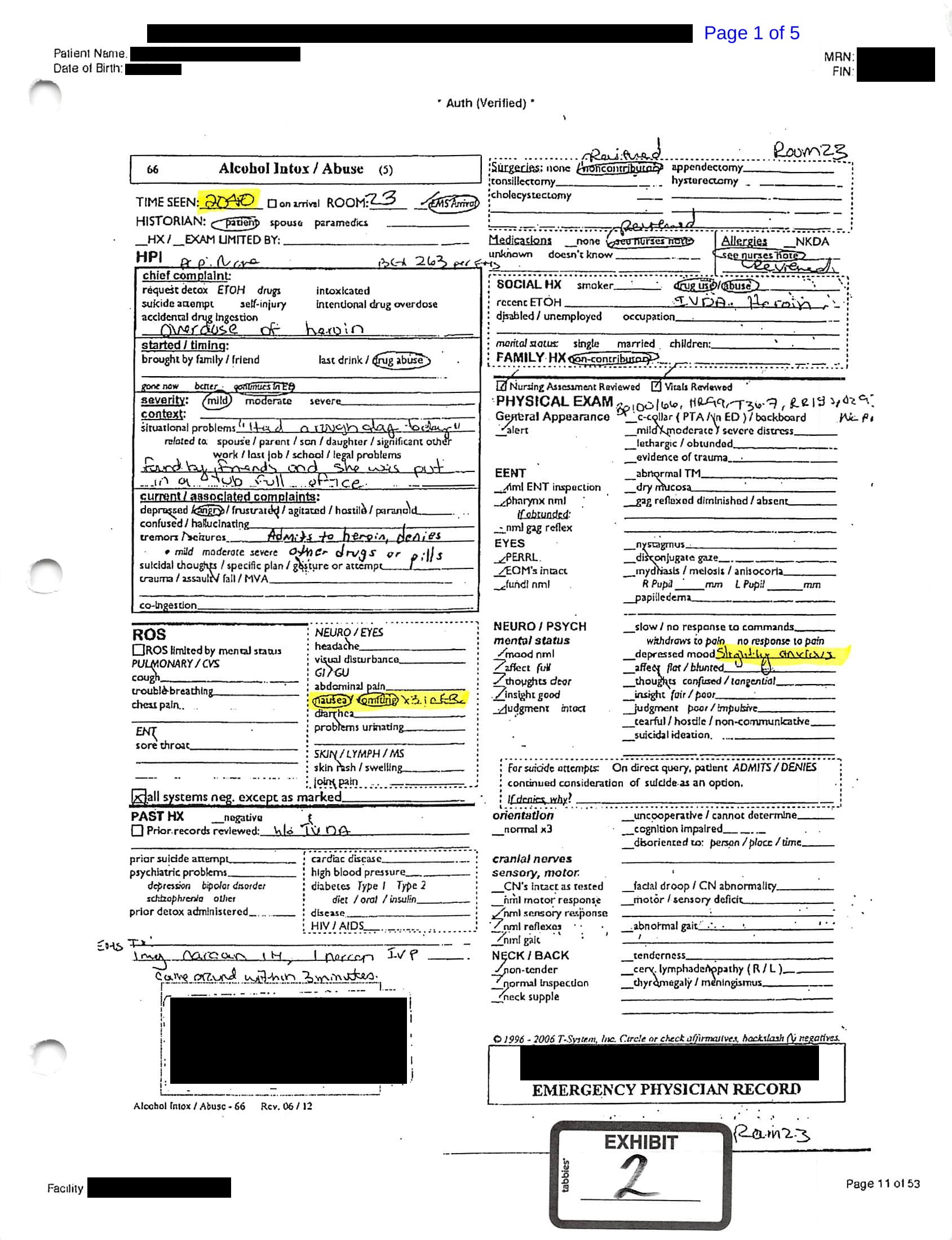
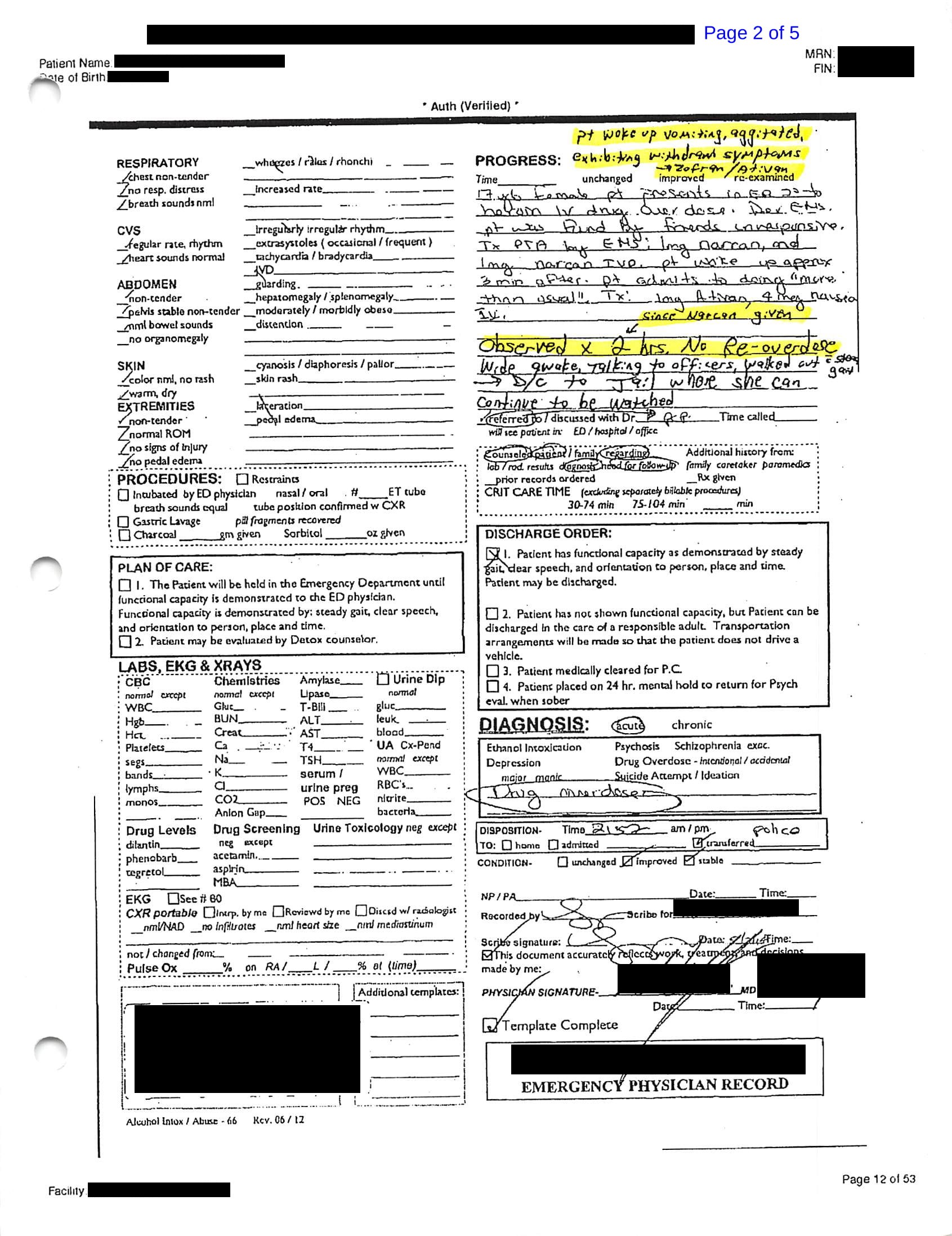
Documentation shows that blood glucose was 263 per EMS. Chief complaint is listed as “overdose of heroin”. The patient reported she “had a rough day today”, and was found by friends and put into a tub full of ice. She reported heroin use but denied other drug intoxication. She seemed angry. The review of system is positive for nausea/vomiting x3 in the ED but otherwise negative. Past medical history is positive for IV drug abuse. The physician documents that 1mg Narcan was given IN (intranasal) and 1mg naloxone was given by IV, and she “came around within 3 minutes”. Surgeries, medications, allergies were all reviewed. Physical exam includes the vital signs at the time of discharge and the fact that the patient feels “slightly anxious” and is otherwise negative. Lab tests were not ordered.

Additional information includes that the patient “admits to doing more than usual”. Due to the anxiety and nausea/vomiting described, she was given 1mg Ativan and 4mg “nausea”. Any reasonable doctor would assume that this means ondansetron, but no exact documentation of this is contained in the record available from the court proceedings. No time of administration is apparent from the documentation we have for review.
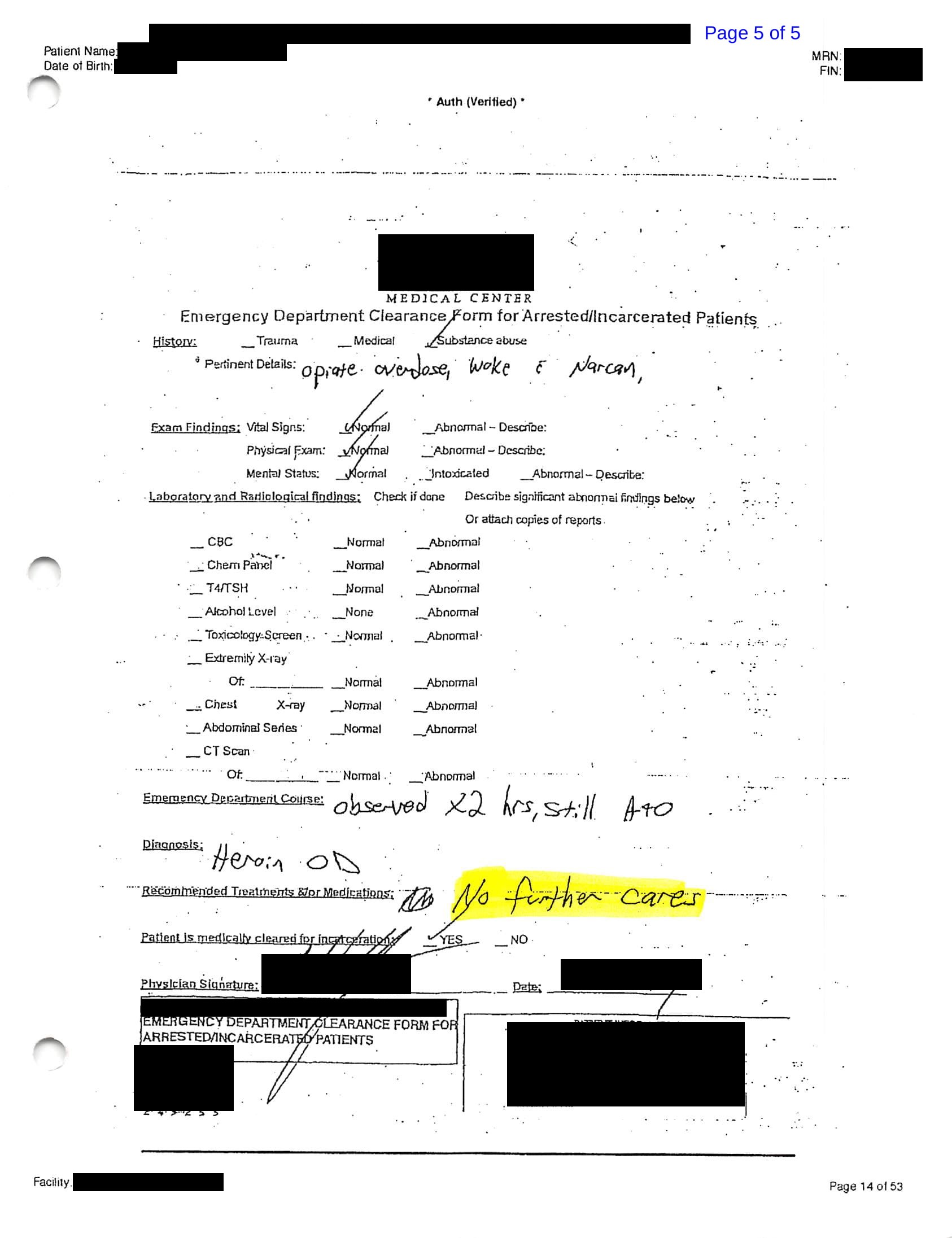
The bottom half of the “Progress” section of the T-sheet contains information that could be best described as the medical decision-making, the most important part of any ED note. It notes that the patient was observed for 2 hours since naloxone was given (naloxone first given at 7:34pm, discharge at 9:52pm). Discharge information shown below:
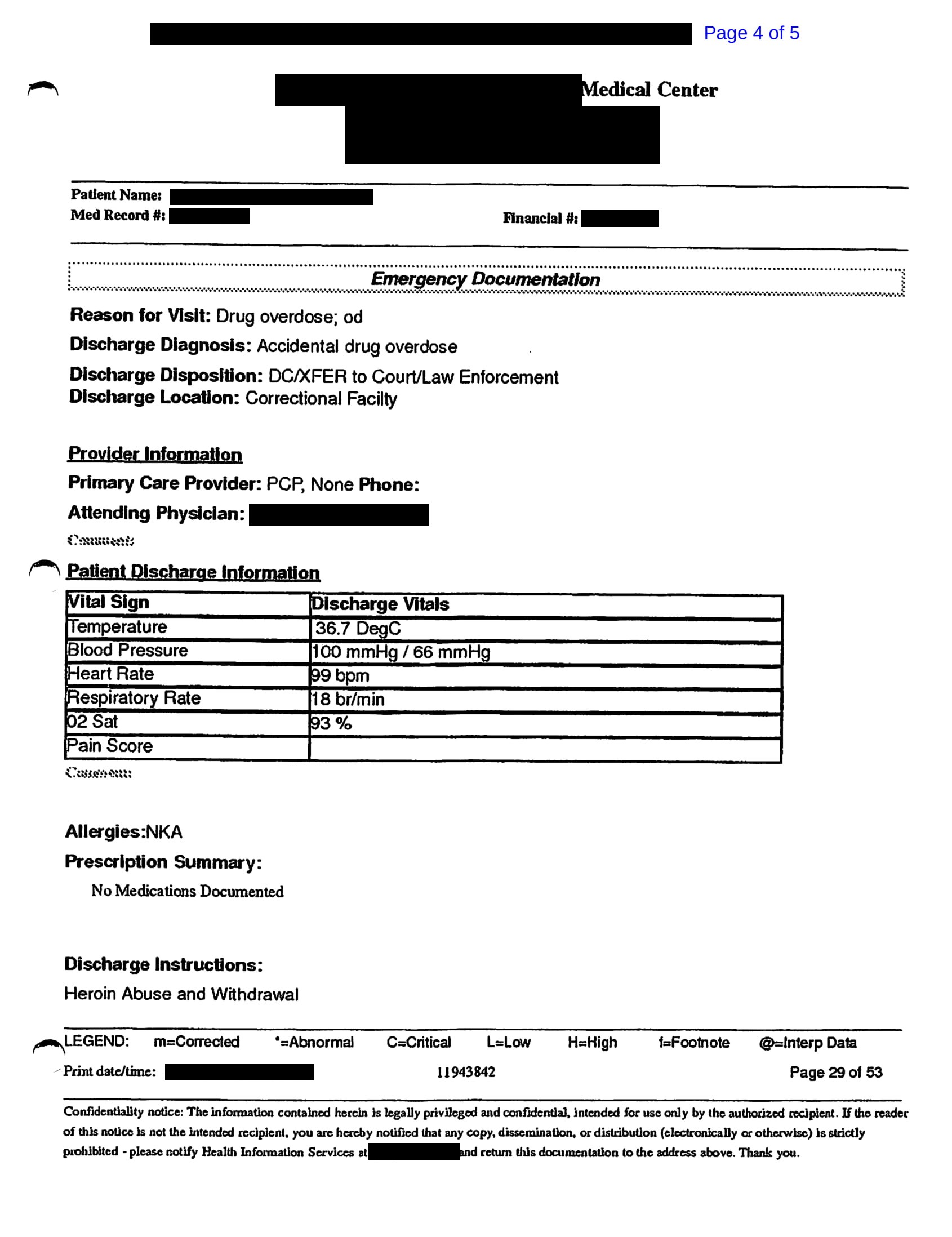
Police that assisted at the scene of the overdose discovered that she had an outstanding warrant for her arrest. Therefore, at the time of discharge from the ED, she was taken into custody. In addition to medical staff who were with her in the ED, her mother, police officers, and hospital security guards were also present.
Her condition is described as “wide awake, talking to officers, walked out with steady gait”. The note indicates: “D/c to jail where she can continue to be watched”. Check box describes that patient has “functional capacity as demonstrated by steady gait, clear speech, and orientation to person, place and time. Patient may be discharged”. Patient was counseled regarding her diagnosis and need for follow-up. Final diagnosis was drug overdose.
At the time of discharge, it is unknown how long she will be in custody or the exact details of how she will be monitored at the juvenile detention facility.
Discharge information and clearance:
A few preliminary comments about this patient’s care thanks to input from Dr. Jeremy Faust:
- Her blood sugar is noted to be 263. This may be normal in a patient with diabetes, but this is a young patient without medical issues aside from recent drug overdose. Does this warrant checking labs, or at the very least, a recheck of her blood glucose prior to discharge?
- The patient received chest compressions, albeit from a lay person who likely does not have much medical knowledge or expertise. Patients who have undergone chest compressions are at risk for pneumothorax, aspiration pneumonia, contusions, among other injuries. Obtaining a chest xray should have been an important part of this patient’s workup.
- The patient’s saturation at discharge is 93%. If this was an elderly patient with COPD, this may be acceptable. However, this is a 17 year old girl without pulmonary disease. Should a saturation of 93% preclude discharge?
What do you think the outcome will be for this patient?
Do you agree with the management of this patient?
How would you have managed the patient’s presentation?
What areas of documentation could be improved?
Primary concern i have with the management of the patient is that they were given a benzodiazepine in the setting of a known opioid overdose. When the naloxone wears off and the effects of the heroin take effect again, it will be compounded by the ativan that was given in the system and result in the patient being found apneic in the jail cell.