Previous Cases (Home Page)
Intro
ED Visit
ED Bounceback
Referral Hospital
Autopsy
Expert Witness Opinions
Legal Outcome
Medical Review
Documentation Review
As in any medical malpractice case, the physician’s documentation is closely scrutinized. Thorough but concise documentation helps lay the groundwork for an effective defense, because it helps explain your thought process to the expert witnesses who are analyzing your care, the attorneys, and possibly the jury. This case contains very little information in regards to explicit description of what the physician was thinking. In previous months the Documentation Rubric has called for specific descriptions of each step. After reviewing more cases and reflecting on the value of documentation, the Rubric has been updated to allow more credit for actions that can be easily and unambiguously deduced from the chart, even if not explicitly described by the physician. This is more reflective of the true practice of Emergency Medicine.
Looking to improve your documentation? Review the Documentation Template here! It is meant to be used while working clinically to help create excellent documentation that can be easily defended. An early blog posts explains further details about using the Documentation Template.
This month’s post received a score of 13.5/20.
Just as in last month’s case, the use of T-sheets has created several challenges for the physician. While they are great for rapid documentation, they are difficult to defend due to various reasons, including limited information, mindless checking of boxes, and poor handwriting.
For easy reference, the T-sheet is listed again here:
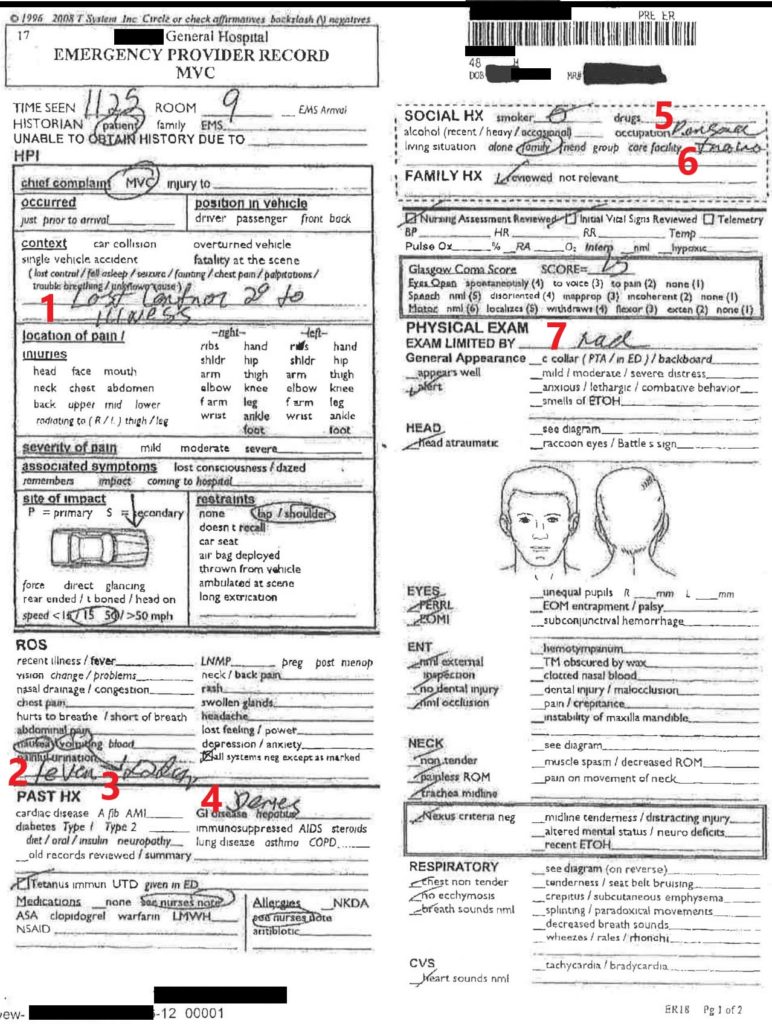
1: Lost control secondary to illness
2: fever
3: x2 days (referring to vomiting)
4: Denies (referring to past medical history)
5: Personal trainer (occupation)
7: NAD (“no acute distress”)
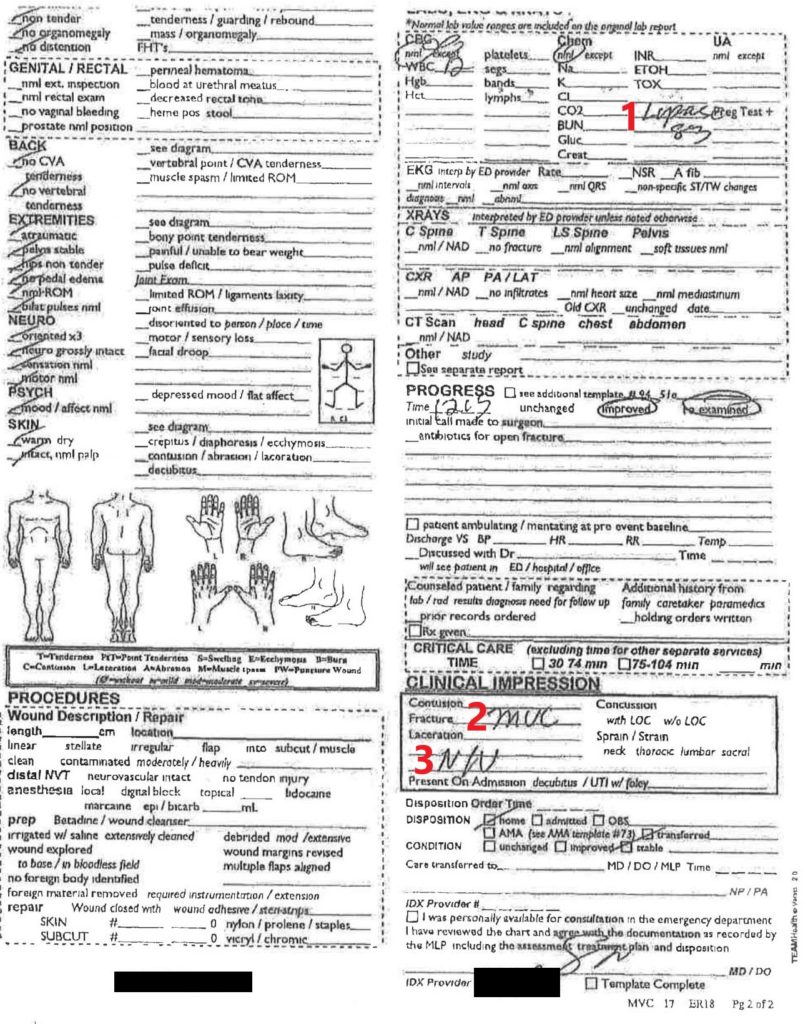
- Lipase 83
- MVC (Motor Vehicle Collision)
- N/V (Nausea and vomiting)
Brief Overview: 1/2
There is no brief overview section in this note. The T-sheet format makes it basically impossible to include a brief overview. While not absolutely necessary, it is a useful tool to help focus the reader on the important parts of the patient’s history. This should be a 1-2 sentence summary. An example for this case: “The patient is a 48 year old man presenting to the ED after a MVC. He was noted to be confused at the scene, is tachycardic and febrile, and has been feeling ill with nausea/vomiting for the past few days”. The goal is establish the relevant facts in their most distilled version. 1 point deducted as the chart makes no mention of the patient’s confusion or presenting tachycardia. The box for “initial vitals reviewed” is checked, which is probably fine if vital signs are normal. Indicating that you have seen any abnormal vital signs is important. Vital signs are…. vital. The T-sheet even provides spaces to record vital signs and it is left blank.
Testing: 2/3
The testing for this patient is fairly logical. CBC, CMP, and urinalysis were ordered. The most useful part of documenting the tests, at least in regards to defensibility, is to explain why you DIDN’T order specific tests. Obviously there are some tests that would be completely ridiculous to order (for example, ordering a DVT ultrasound would make no sense in this situation), and this does not require any specific documentation. But tests that are on the border of what could be reasonably ordered are high yield documentation points. For this patient, explanation of why no imaging was done could have been beneficial. In the article reviewing this patient’s medical care we discussed why head CT for trauma imaging was not necessary; this discussion could easily be distilled into one sentence and included in the rationale of the testing. If you thought about ordering something and decided against it, it is wise to include your rationale in your note.
Therapy: 3/3
The therapy section is one area where deduction from the chart is necessary, rather than expecting explicit documented reasoning. This patient was given fluids, ketorolac and promethazine, which are all logical orders based on the documentation. A key point is to document the response to therapy. In this case the physician circled “improved” on his re-examination. He could have elaborated on the improvement further but given the demands of a busy ED this is not always possible.
Differential: 4/8
This physician undoubtedly had a broad differential in mind when seeing this patient. Based on the orders we can tell he considered anemia, dehydration, renal failure, various electrolyte disturbances, urinary issues such as hematuria from trauma or possibly a UTI underlying his presentation, among others. It would have been wise to mention that various traumatic injuries are initially on the differential for this patient as well but that they could be ruled out with history/physical. It is also wise in any trauma to indicate that you have considered underlying medical causes, even if you ultimately do not think the trauma had a medical etiology and it needs no further workup. While the true cause of the patient’s accident and ultimate demise may not have been on the mental differential of the physician in this case, it is very unlikely that it would have been considered by most physicians seeing this patient without the benefit of a retrospectoscope.
Discrepancies: No deduction
Only minor discrepancies are noted. For example, the triage nurse noted GCS 14 while the physician noted GCS 15. His GCS may have changed in the interim between triage and physician evaluation, so this is not surprising. The attorneys in this case did not use this to attack the healthcare team, but discrepancies are often used in this manner. No points were deducted because the difference between GCS 14 and GCS 15 is likely inconsequential in this case.
Aftercare: 3/4
The discharge information hit many of the key elements of aftercare: plan of care, follow-up, and return precautions. The plan of care is to have the patient eat a bland diet, avoid dairy, and rest. Return precautions were given in the discharge paperwork, as was a vague statement about following-up with another physician. Areas of concern include the fact that there was no timeline in regards to follow-up, and no specific instructions on which physician to follow-up with. The more clear and individualized the follow-up instructions are, the more credible they seem. Vague, impersonal statements that are printed off and handed to every patient as they walk out the door are often discarded. If you want your patient to actually follow your instructions, telling the patient your recommendations with a face-to-face conversation is the most effective way. Templated discharge papers work best as a supplement or additional reminder in addition to what the physician has verbally told the patient. Documentation of this discussion can make the aftercare even more defensible.