This case illustrates a rare but well-known disease with catastrophic consequences. Emergency Medicine residents are frequently tested on aortoenteric fistula, but to diagnose one in real practice remains quite uncommon.
The first step in making the diagnosis is being aware that it is a possibility. Any patient presenting with possible GI bleed and a history of aortic surgery should raise a red flag in the clinician’s mind. In this case the resident knew that it was a possibility, but did not arrive at the diagnosis.
CT Scan Contrast
One seemingly critical issue was the decision to order a CT scan without contrast. Using contrast would have given the radiologist a greater chance to identify bleeding from the aorta. During her deposition, the resident mentions that the patient’s presentation seemed more classic for kidney stone, which is why a non-contrast renal stone protocol CT was ordered. Given the fact that a kidney stone is a much more common cause of pain than aortoenteric fistula, it could have been a reasonable plan to start with a CT renal stone protocol. However, especially in light of the patient’s history of aortic surgery, it would be prudent to then proceed with a contrast study. Alternatively, a CT abd/pelvis with and without contrast could be done to expedite the workup.

Hemoglobin: Continuous Bleed vs Herald Bleed
Most bleeding complications in the ED are acute and continuous. These types of bleeds are seen in most traumas and GI bleeds. Encountering an intermittent bleed (such as a herald bleed) is much less likely, but is just as important to identify. It may be the only chance a physician has to recognize that a patient has an impending catastrophe.
This case illustrates the importance of detecting a hemoglobin drop, especially from a herald bleed. The plaintiffs point out that the patient’s hemoglobin had dropped from 14.6 in January 2006, to 10.2 on the day he was discharged from the VA Emergency Department.
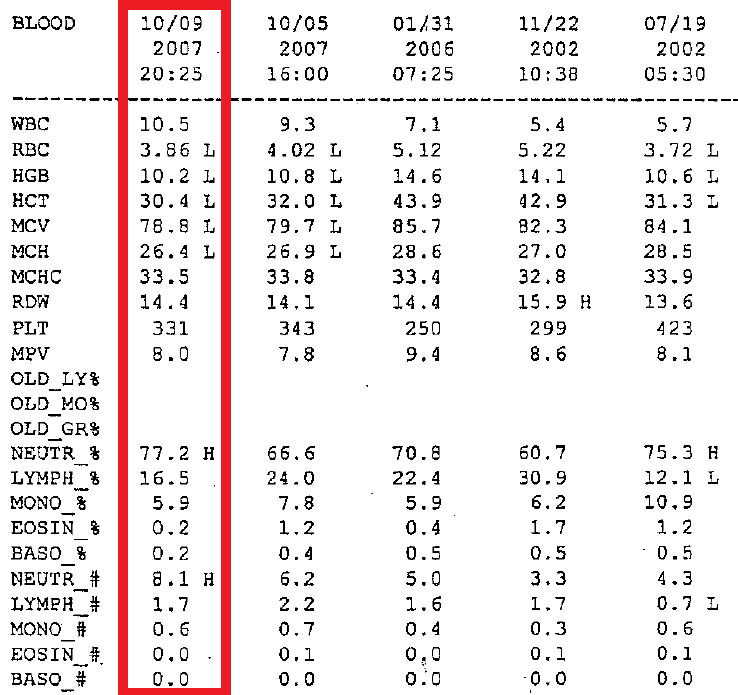
The resident had noted that there was only a small drop compared to the PCP visit several days earlier. At first glance this may seem reassuring. If he was having an acute and continuous bleed, a much bigger drop would be expected over the course of 4 days. The resident likely felt reassured that the drop from 14s to the 10s was not a recent change, because a continuous bleed would likely have caused the hemoglobin to continue to drop over the interim 4 days. However, this theory holds less weight in a disease process where there may be a herald bleed. With a herald bleed, there may be a small drop in hemoglobin that stabilizes for a few days or weeks, followed by catastrophic and fatal bleeding.
In fact, the mean time from herald bleed to diagnosis of an aortoenteric fistula is 14 days in one study, with a minimum of 4 days. During this time frame there may be an initial drop in hemoglobin, followed by a period of stabilization, then sudden exsanguination and death.
In patients who are at risk for a disease that can cause a herald bleed, do not be falsely reassured by a hemoglobin that stabilizes.
Another issue is the utility of a hemoccult in GI bleeding. The hemoccult test is used to screen for blood in the stool. This is most applicable in the primary care setting and may be used as a part of colorectal cancer screening.
In the ED, the hemoccult has been maligned as an unnecessary and overused test. The ED is in the business of diagnosing life-threatening GI bleeding as opposed to occult bleeding. Most life-threatening GI bleeds result in gross blood on rectal exam, in which case a hemoccult is not necessary. A GI bleed (generally expected to be a continuous bleed) that does not cause any gross blood on rectal exam likely does not need admission and can be discharged for outpatient follow-up.
However, in the case of an intermittent bleed like a herald bleed, a small amount of occult blood may provide an important clue. If a patient is at risk for aortoenteric fistula, a positive hemoccult can provide a small piece of information that may help direct the physician toward the diagnosis. On the other hand, an AEF can still occur with a negative hemoccult test, so a negative result is not necessarily reassuring.
Continue to the next page to see the documentation assessment.