The purpose of this website is to improve doctor’s medical knowledge and documentation by reviewing real-life malpractice cases. This article will review the documentation of the physician who was sued. There are three goals of documentation: defensibility, continuity of care, and billing. This post will focus primarily on the defensibility aspect of documentation. I have created a Documentation Rubric that will help guide the grading of this note. I have also created a Documentation Template to help physicians write defensible notes.
Home Page
Post 1: Introduction
Post 2: Bad Outcome
Post 3: Legal Outcome
Post 4: Documentation Review
Post 5: Medical Review
This post will review the documentation of the initial doctor who saw the patient and apparently misdiagnosed a PE as bronchitis. As mentioned above, I’ll be using the Documentation Rubric to help grade and assess what was written. As an overall statement, I’ll say that this was a difficult one to read and grade. Any board-certified EM doctor should have seen the bad outcome coming from a mile away, and the documentation did this doctor no favors. It is sparse and contains almost no insight into any of his decisions or thought process. The defensibility of the chart lies in the Medical Decision-Making (MDM) portion, not the history/exam/ROS/PMH/orders, etc… and unfortunately there is basically no MDM section in this note. I’ll attempt to grade the documentation in isolation, without dragging the poor medical decision-making into this (we’ll save that for the next post).
This chart achieved a score of 6/20 on the Documentation Rubric.
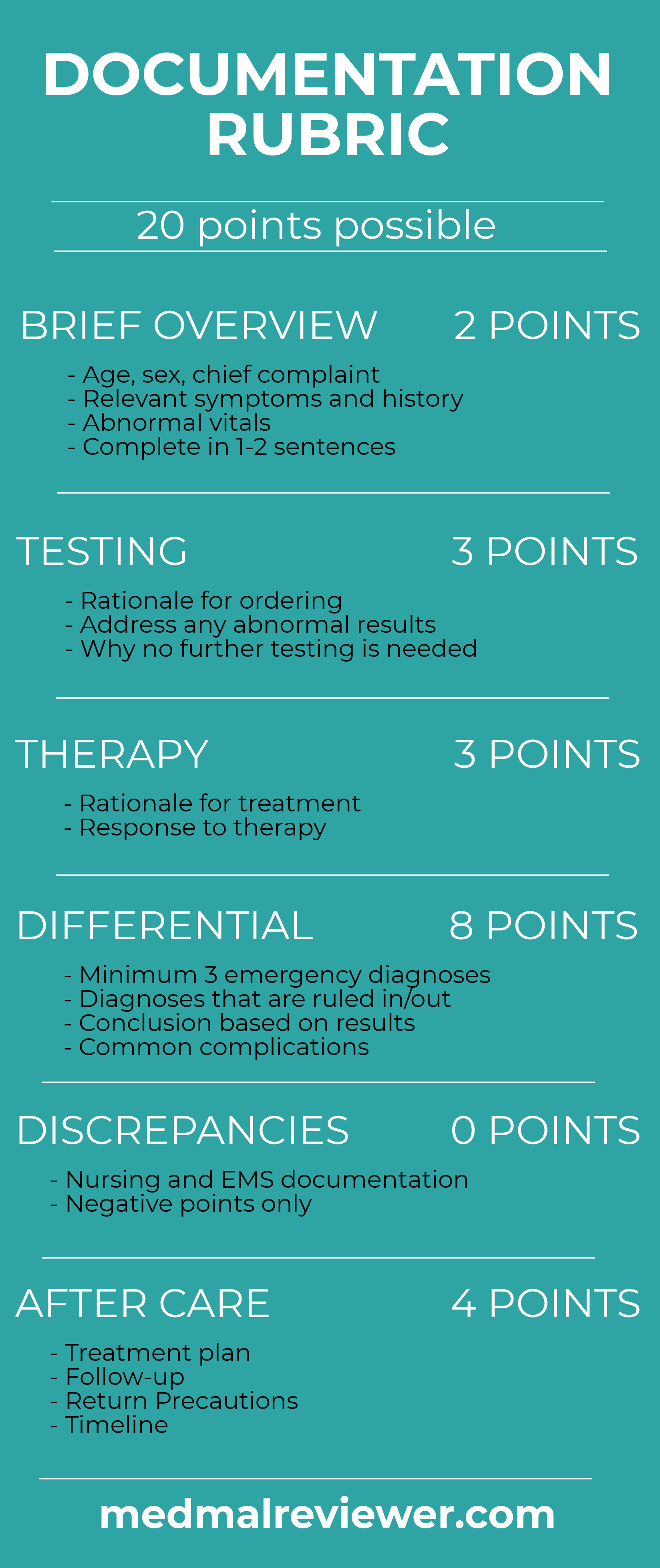
Brief Overview: 0.5/2
The brief overview sets the stage for the rest of the MDM. It gives us the basic introduction to the patient, their presentation, any relevant history and initial vitals. This information is found scattered throughout the chart, but it is useful to synthesize into one brief statement at the beginning of your MDM, rather than leaving it randomly scattered throughout your note. In this note, the closest thing to the brief overview is found at the very beginning, under chief complaint/history of present illness.
There is no MDM section here, but this initial description does mention some of the basics of a brief overview: shortness of breath and back pain, and some vitals. This could be better if it had included a few of the other relevant symptoms (chest pain). A brief overview section is also better served by mentioning the abnormal vital signs (febrile, tachycardic, tachypneic) rather than letting some software autopopulate them into the note. Given that there is no true MDM section, lack of mention of other relevant symptoms (chest pain), and no discernable emphasis on the abnormal vitals, we will assign 0.5/2 points.
Testing: 0/3
The testing section is an analysis of the physician’s explanation for ordering various tests, acknowledging or addressing any unusual results, and explaining why no further testing is needed. Most testing decisions are fairly obvious. If an old man with a history of heart attacks has chest pain, you don’t need to wax poetic about why you’re ordering troponins and an EKG. Its obvious. But if you order something unusual, or make an odd decision in regards to testing, you better explain it in your note. This visit contained exactly that: unusual testing and an odd decision in regards to testing. There is a complete failure to explain it. We can deduce from the chart and later depositions what happened, but this is not the ideal avenue for explaining your though process. Judging from the time stamps, a D-dimer was ordered, immediately followed by ultrasounds and CT scans. If you’re not going to wait for the dimer, why order it anyway? And if you’re going to order a CT scan, why get an ultrasound? Did the ultrasounds get ordered because the physician thought the right leg erythema could be a DVT? Did they order the CT scan, cancel it after finding out they couldn’t get it, then order ultrasounds as a sort of compromise? We’ll never be sure because there is no explanation from the doctor. And not only is there no explanation, its impossible to even guess at the logic. I don’t see any way I can charitably give even half of a point on this.
Therapy: 1.5/3
In any good MDM, we expect to see a brief explanation of the treatment ordered, and ultimately a response to treatment. Again, if the thought process is obvious, no need for any long explanation. If the patient is severely dehydrated and you give fluids, you don’t need to write much, if anything. In this case, I can make some assumptions about the medications that were given. Ketorolac can safely be assumed to be treating this patient’s pain. It’s a reasonable choice. Tylenol can safely be assumed to treat pain and treat the patient’s fever. Anti-fungal can logically be explained given the suspicion for a fungal infection. Doxycycline is a bit harder to explain given rates of resistance and the fact that it seemed to be more suspicious for fungal infection than bacterial cellulitis, but its not unreasonable to treat for both fungal and bacterial sources if unsure.
One area for improvement here is the failure to document the improvement with these. There is a brief mention of “Condition: improved” in the disposition section, which will garner a half point. But this is really not sufficient. What is improved? Did the pain improve? The changes in vital signs are recorded at least somewhere, buried within the nursing documentation. They show that some of his vital signs have improved. However, the patient is persistently tachycardic at discharge, which is a major red flag. I’ll give some points for my ability to logically deduce what he was thinking with the medications, but deduct for no explicit description of any of these decisions and lack of more thorough explanation of the improvement in condition.
Differential: 2/8
The differential is the core of your medical decision-making. It guides everything you do, even when you’re not explicitly thinking about it. Sometimes our brains can immediately jump to the diagnosis and form a differential of one item, which is sometimes right, but sometimes wrong. Writing out a differential is an excellent way to spur yourself to thoroughly think through a case. It would have served this physician well. Unfortunately there is no mention anywhere of a differential. There is a clinical impression at the end with a few diagnoses, and that’s it. A good differential could include things that any board-certified EM doctor would think of after hearing the Brief Overview, things that have been ruled out based on history/exam, common complications of diagnoses given, etc… There is no rationale explained for why various diagnoses have been ruled out or ruled in. The only place we see even a hint of a differential is in regards to the erythema on the right toe. The clinical impression lists “Cellulitis/Tinea Pedis”, which I suppose could be considered a 2-item differential for the erythema. It is an insufficient differential even if it was the only complaint. We can logically deduce that the physician thought this could be a PE based upon the D-dimer, ultrasounds and attempt at ordering a CT. But apparently it was not high enough on the differential to warrant any further work after the CT was cancelled. I’ll be generous and give a point for a 2-item differential for foot erythema and a point for my attempt at reading this doctor’s mind to know he was thinking about PE.
Discrepancies: No point deduction
Good documentation avoids discrepancies between the various people who are writing notes. Mostly commonly this means comparing the doctor’s note to the nurse’s note and EMS note. There’s not EMS note (for the first visit) so we’re off the hook there. The nursing note mentions that respirations are “mildly labored” initially, then “unlabored” after reassessment. The physician’s note reports the respirations to be non-labored. This is a minor difference that could be easily explained by seeing the patient at different times or just a difference in judgment. I don’t think that the physician would have changed his plan even if he had seen this. Its tempting to deduct a point here (the discrepancies section can only be used to deduct points) but the difference in assessment is not large and likely would not have had any ultimate impact on the patient’s care.
Aftercare: 2/4
Whenever a patient is discharged from the ED, the plan of care must be clearly laid out. This physician made a reasonable attempt at the aftercare and its documentation, if considered in isolation and ignoring the big miss of a fatal diagnosis. Remember, we’re grading the documentation here, not the medical care. There is a treatment plan laid out with multiple medications. The follow-up is somewhat lacking. There is no clear documentation that he asked the patient to follow-up in a few days for a CT scan if not improving. If you’re worried enough about a PE to attempt to scan them, it would be a wise idea to at least document that you told them to follow-up if not improving. But its not present. Discharging this patient is already incredibly dangerous, not documenting the follow-up plan and what you told them is like pouring gasoline on the fire. Return precautions are mentioned in regards to returning to the ED immediately if symptoms worsen or fail to improve. Unfortunately most of the physician’s documentation is obviously autopopulated and it makes the reader very dubious that this information was actually discussed with the patient. Writing what exactly was discussed with the patient would have been helpful here. The patient was given discharge papers with basic information about medications and returning to the ED if needed, but obviously most patients never read this and its obvious to anyone (most importantly, the jury) that its more of an (failed) attempt at protecting the physician than serving the patient. This physician’s EMR helped him somewhat and hurt him somewhat with this section. It makes it easy to autopopulate statements about the aftercare, but also makes every reader suspicious that the sentences are just there because he clicked some buttons, not because he actually did what was written.
Overall, this chart scores 6/20. It’s a bad score for a bad note. The fact that it doesn’t even have a medical decision-making section is problematic, and it’s an issue likely exacerbated by the doctor’s EMR. There’s basically no explanation of the doctor’s thought process besides conjecture and inferences. Don’t leave your documentation in the hands of a jury with only the conjecture and inferences of lay people to defend it. This note could be significantly improved by using the Documentation Template. Not only would it have made the note easier to defend at trial, it may have nudged the doctor towards better care that could have saved a patient’s life, in addition to stress and money. The Template isn’t a magical panacea that will instantly create perfect notes or perfect medical care, but it will help you improve your notes in a systematic and concise way that could help you avoid a similar situation.