Index Case 8
Cough
Follow-up
Specialty Consult
Tumor Board
Legal
Review
Documentation
The initial urgent care documentation will be assessed with the Documentation Rubric. The Rubric and Template were created specifically for EM notes, but they apply equally well to any undifferentiated patient with an acute complaint.
The Documentation Template was created for clinicians to use while working, in order to create defensible documentation. This is specifically focused on the medical decision-making (MDM) portion of the note, not the history, social/family history, past medical history, exam or ROS. The Documentation Rubric was created for grading MDM sections.
The note for this case is again shown here.
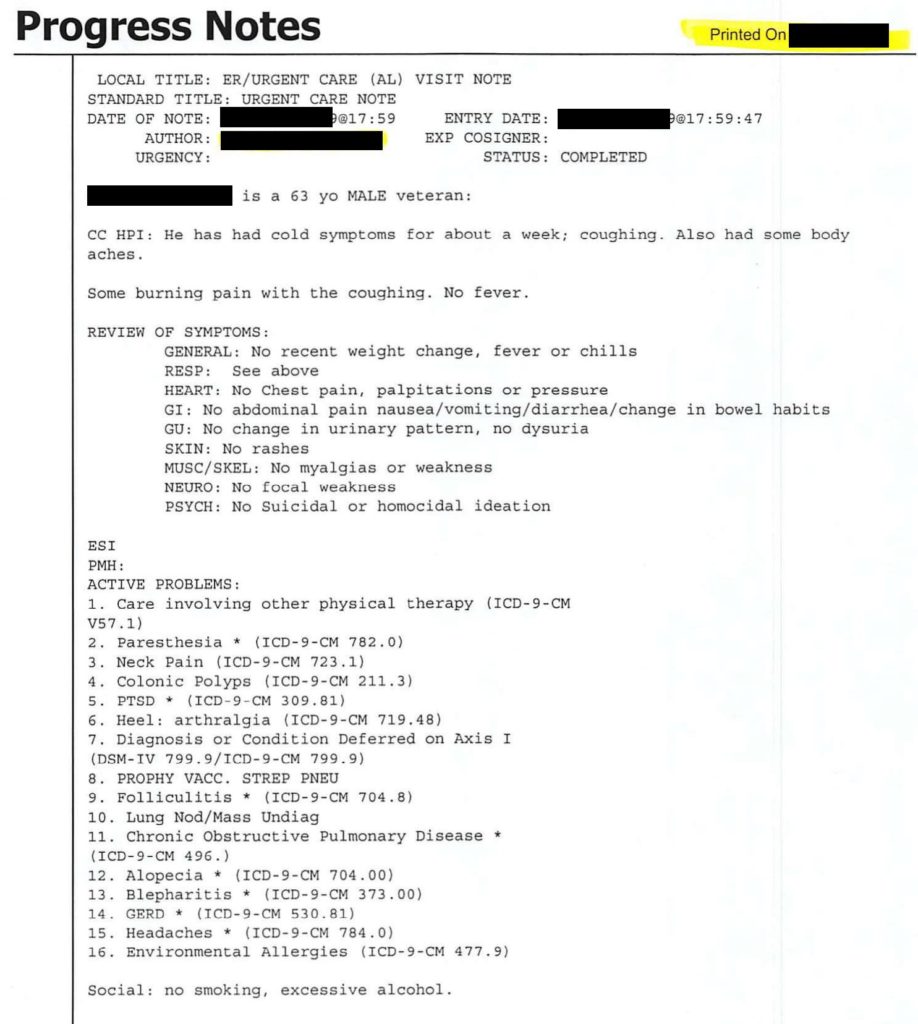
The physician’s note earned a score of 5/20.
This note is very poor. The rubric is meant to assess the MDM portion of the note, which in this case is just a few lines that barely show any thought process. There is almost nothing here that can be graded. Even though this rubric was built for EM documentation, it can easily be applied to any undifferentiated complaint. Writing notes that are this brief and devoid of thought-process places the physician in a very fragile place if the care is ever questioned or examined.
Brief Overview: 0/2
The H&P is so brief it barely even qualifies as a brief overview. The brief overview should be 1-2 sentences explaining the patient’s presentation. In this case, the H&P barely even rises to this level, let alone having this listed at the start of an MDM section.
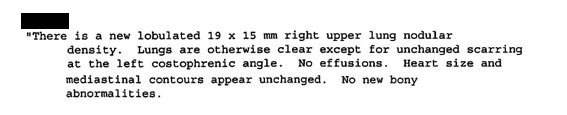
Testing: 0.5/2
The physician mentions a chest x-ray was ordered. There is no mention of why other testing that might commonly be done for a patient with a cough was not needed. The fact that he summarized the patient’s result initially seems encouraging, until we realize that he was grossly incomplete in his summary. Including a summary of the relevant findings (not a copy/paste of the results) is helpful, but this presumes a correct and thorough understanding of the results.
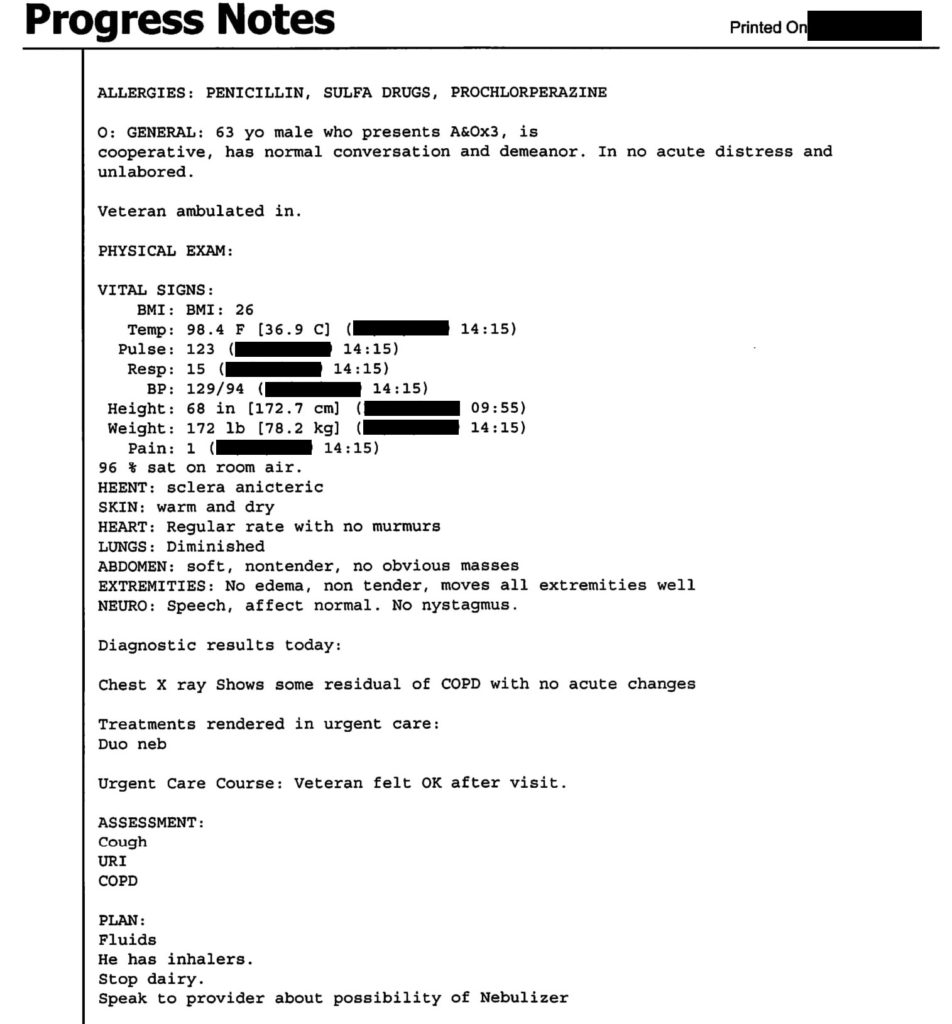
Therapy: 1.5/3
The patient is given a Duoneb, which is logical given patient’s history of COPD and his current cough. There is not a direct assessment of his response to the Duoneb, but there is a mention that he felt “OK after visit”. Mentioning a response to treatment or a reassessment is a wise idea but this is so vague and nonspecific it is basically useless.
Differential: 2/8
There is a very brief differential listed under the “assessment” section. It includes cough, URI, COPD. He ordered an x-ray, and could have easily mentioned a few things that can be assessed on an x-ray, including pneumonia or pneumothorax. There is no mention of emergency diseases that could cause a cough with burning sensation, body aches, and cold symptoms.
Discrepancies: None
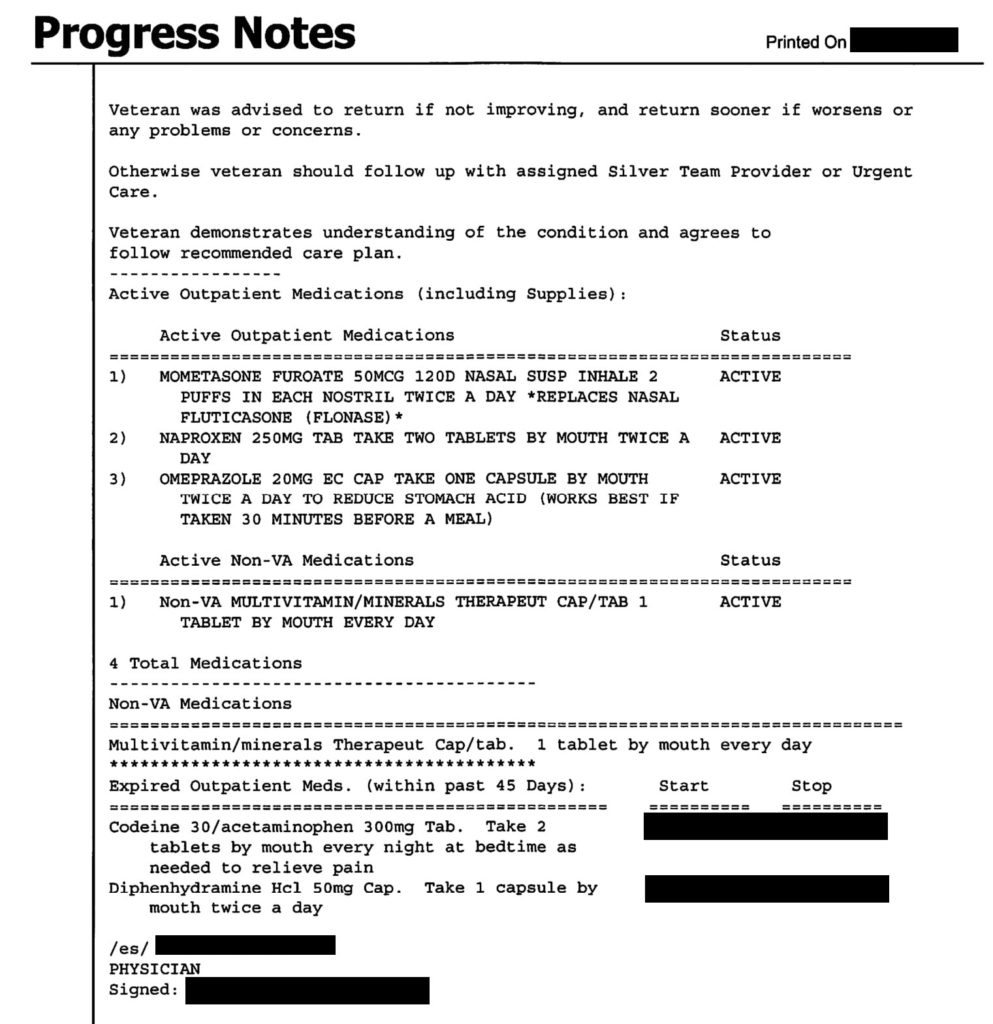
Aftercare: 1/4
The treatment plan is particularly odd in this case. “Fluids” is part of the recommendation, but there is no mention of dehydration or any clear issues that would require extra fluid intake. The patient has inhalers but there are no clear instructions on how he should use them; if he should continue as prescribed, increase the frequency, or stop one. He was told to stop dairy for no apparent reason (what is it with malpractice lawsuits and recommending to stop dairy?).
He was told to return if his condition was not improving or if it worsened, although no time frame was mentioned. Most damning, is that he was told to follow-up but with no clear instructions for why, nor when he would need follow-up. Technically, the patient did in fact follow-up as instructed; seeing a primary 3 years later was within the recommendations he was given. Follow-up and return precautions need clear time guidelines. There is a chance that the physician’s oversight could have been caught at a post-urgent care follow-up visit.
The poor and extremely limited documentation in this note likely reflects the limited and cursory review of the patient’s chest x-ray result and consideration of his follow-up instructions. While the case was dismissed for being outside the statute of limitations, this documentation would have been nearly indefensible at a trial. Do yourself a favor, use the Documentation Template. It might help avoid a poor medical or legal outcome.