Welcome to medmalreviewer.com! The purpose of this site is to improve doctor’s medical knowledge and documentation by reviewing real-life malpractice cases. These cases are presented in long form, deep dive fashion, published monthly. Each case is broken down into several posts. To see more info about the website, here are links to the About Page and FAQs. Another helpful overview post is the 3 Goals of Documentation. I’ve created a Documentation Template to help doctors write notes that are easy to defend, and a Documentation Rubric to grade notes from malpractice cases.
Case 6 Index:
Respiratory Arrest
Outcome
Lawsuit
Depositions
Legal Outcome
Medical Review
Documentation Review
This month’s case is about a 52 year old woman who presented to an ED with shortness of breath. She was seen by a triage nurse and immediately found to be critically ill.
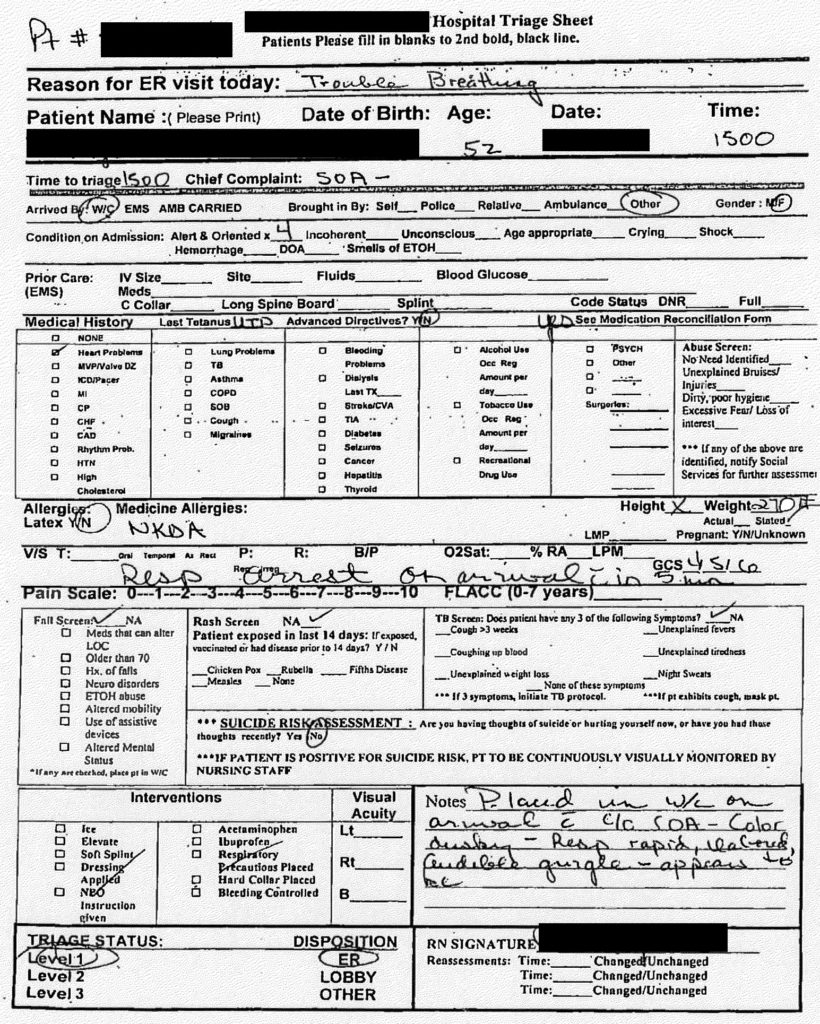
The patient presented with severe respiratory distress, and clearly needed to be intubated. She unfortunately had a respiratory arrest and was completely apneic. She was rushed from a hallway bed into an ED room. There was almost no time to conduct a history prior to her respiratory arrest. The hand-written code sheet is shown below, with text below for clarity.
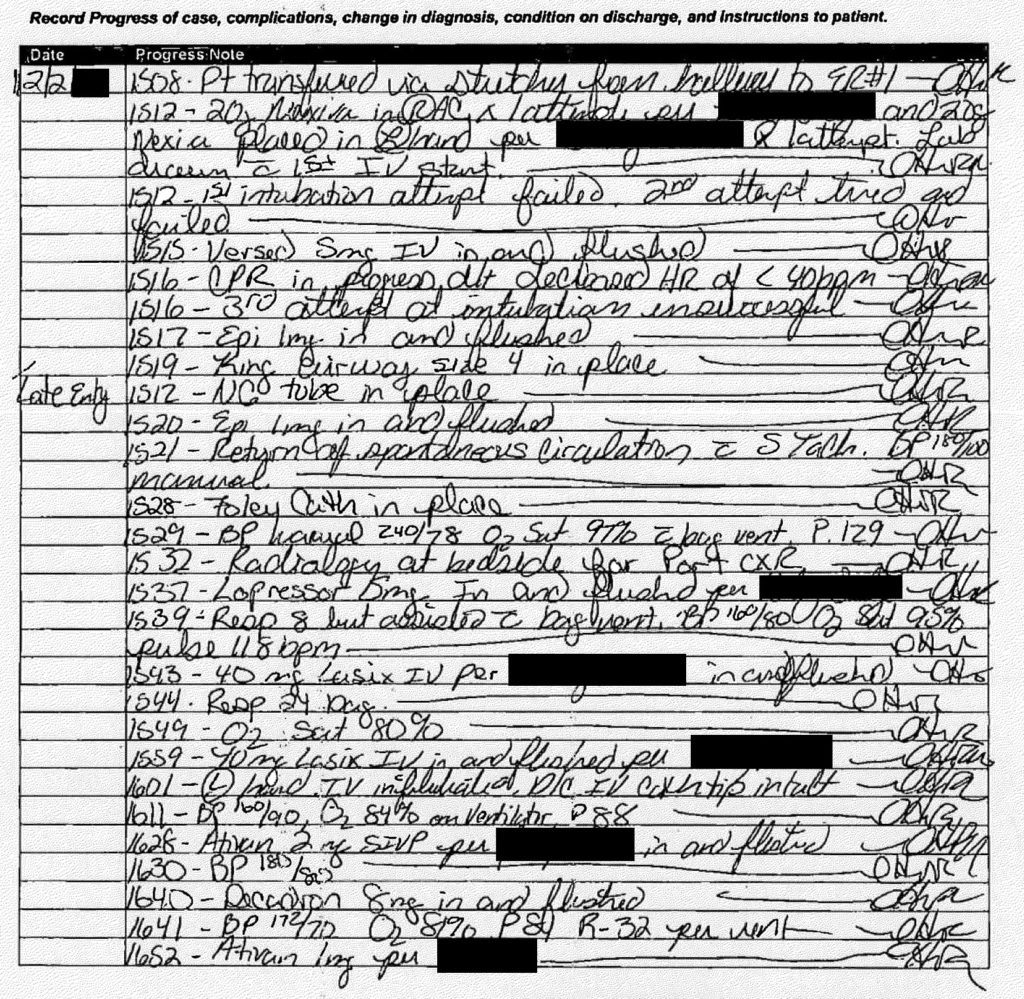
1508 – Pt transferred via stretcher from hallway to ER#1
1512 – 20g Nexiva in R AC x 1 attempt per [nurse] and 20g Nexiva placed in L hand per [nurse] x 1 attempt. Lab drawn with 1st IV start.
1512 – 1st intubation attempt failed. 2nd attempt tried and failed
1515 – Versed 5mg IV in and flushed
1516 – CPR in progress d/t decreased HR of <40bpm
1516 – 3rd attempt at intubation unsuccessful
1517 – Epi 1mg in and flushed
1519 – King airway size 4 in place
Late entry 1512 – NG tube in place
1520 – Epi 1mg in and flushed
1521 – Return of spontaneous circulation with sinus tachyardia, BP 180/100 manual
1528 – Foley cath in place
1529 – BP manual 240/78, O2 sat 97% with bag vent, P129
1532 – Radiology at bedside for port CXR
1537 – Lopressor 5mg in and flushed per [nurse]
1539 – Resp 8 but assisted with bag vent BP 160/80, O2 sat 95%, pulse 118bpm
1543 – 40mg Lasix IV per [nurse] in and flushed
1544 – Resp 24 bag
1549 – O2 sat 80%
1559 – 40mg Lasix IV in and flushed per [nurse]
1601 – L hand IV infiltrated, D/C IV cath tip intact
1611 – BP 160/90, O2 84% on ventilator, P88
1628 – Ativan 2mg IVP per [nurse] in and flushed
1630 – BP 180/80
1640 – Decadron 8mg in and flushed
1641 BP 172/70 O2 81% P84 R 32 per vent
1652 Ativan 1mg per [nurse]
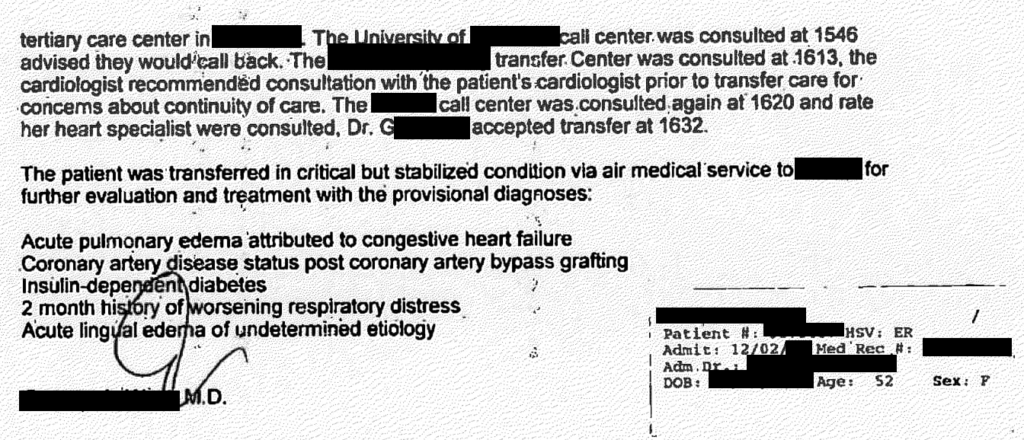
The physician caring for the patient dictated a note, describing the events of her care.
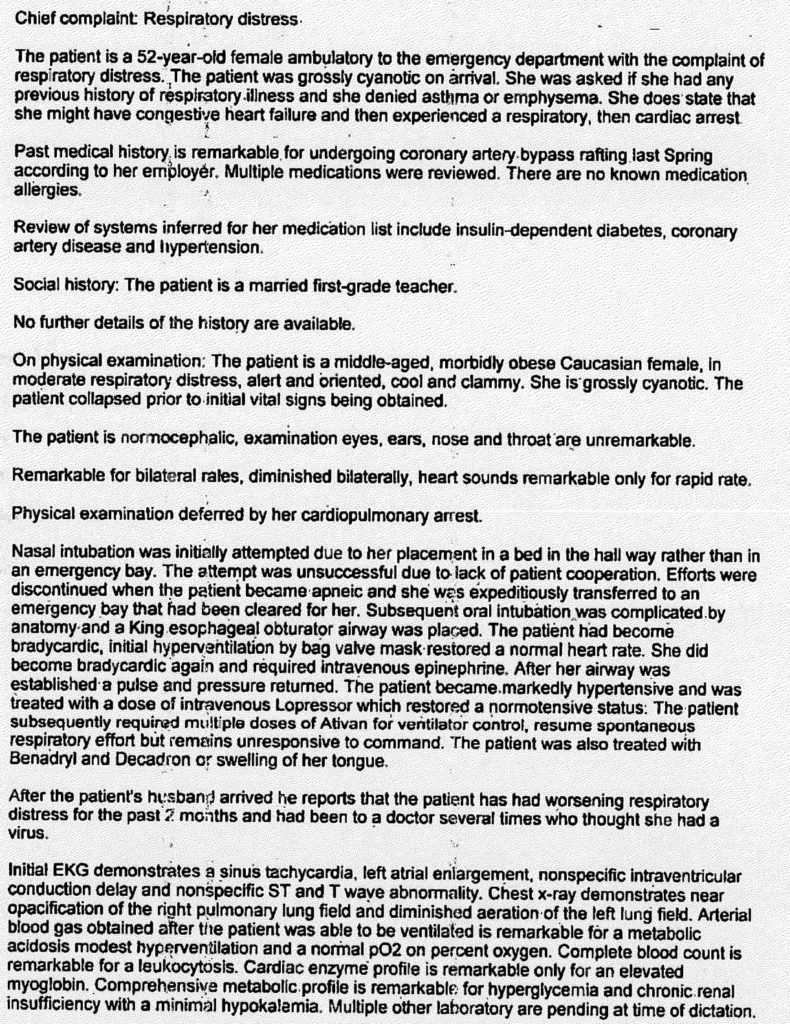
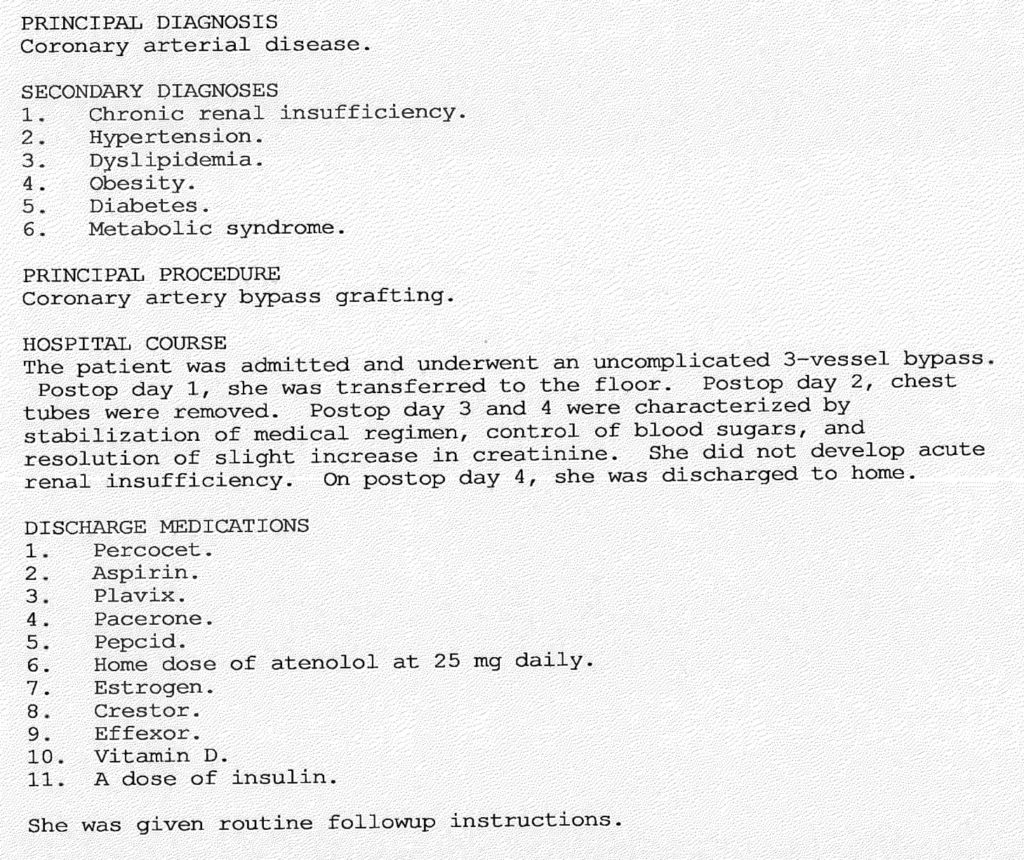
The EKG and lab results are unfortunately not included in the court documents. The hospital was very small and did not have the capability to take care of this patient beyond the ED. Therefore the physician began the process of transferring her to another facility. In the meantime, outside records were obtained. The discharge summary from her CABG was obtained, which was from ~18 months prior to her respiratory arrest.

The physician had to make several phone calls in order to find a hospital that would accept the patient. He first called a regional medical center, where he spoke with another ED physician, Dr. H. After reviewing the case, Dr. H. felt that the patient may need an academic medical center, and recommended transfer to the nearby University. The University’s call center took the patient’s information and reported that they would call back. After not hearing anything back for about 30 minutes, a second regional medical center was contacted. A cardiologist at the second regional medical center recommended consulting the patient’s outpatient cardiologist prior to transferring her. Finally, the original regional medical center was contacted again, and a cardiologist (Dr. G) accepted the patient.

Continue to the next page to see the outcome of this case.
You ought to be a part of a contest for one of the greatest blogs online.
I am going to highly recommend this web site!