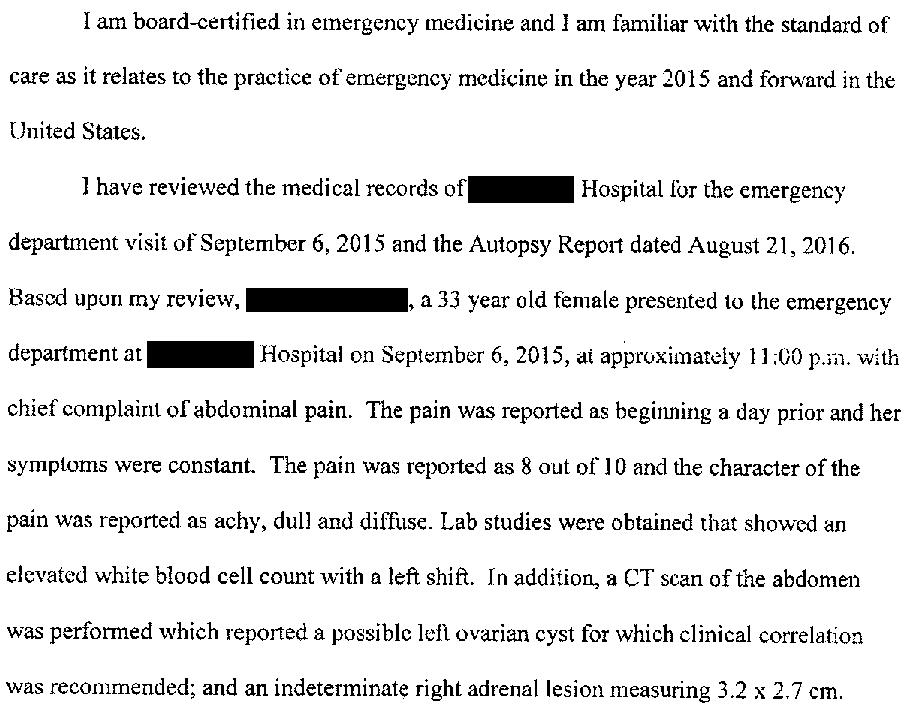
A 33-year-old woman presented to the ED in September 2015.
She reported lower abdominal pain and urinary discomfort.
A pelvic exam was felt to be indicative of PID.
A CT scan showed several findings:
Left ovarian cyst
Gallbladder sludge
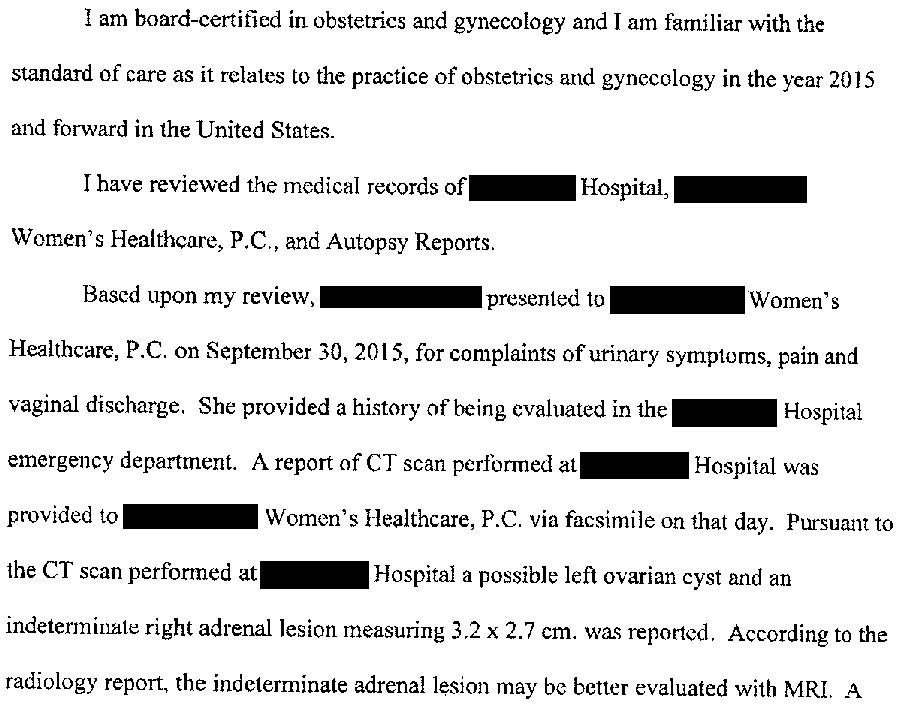
Indeterminate right adrenal lesion, 3.2 x 2.7cm, may be evaluated further with MRI.
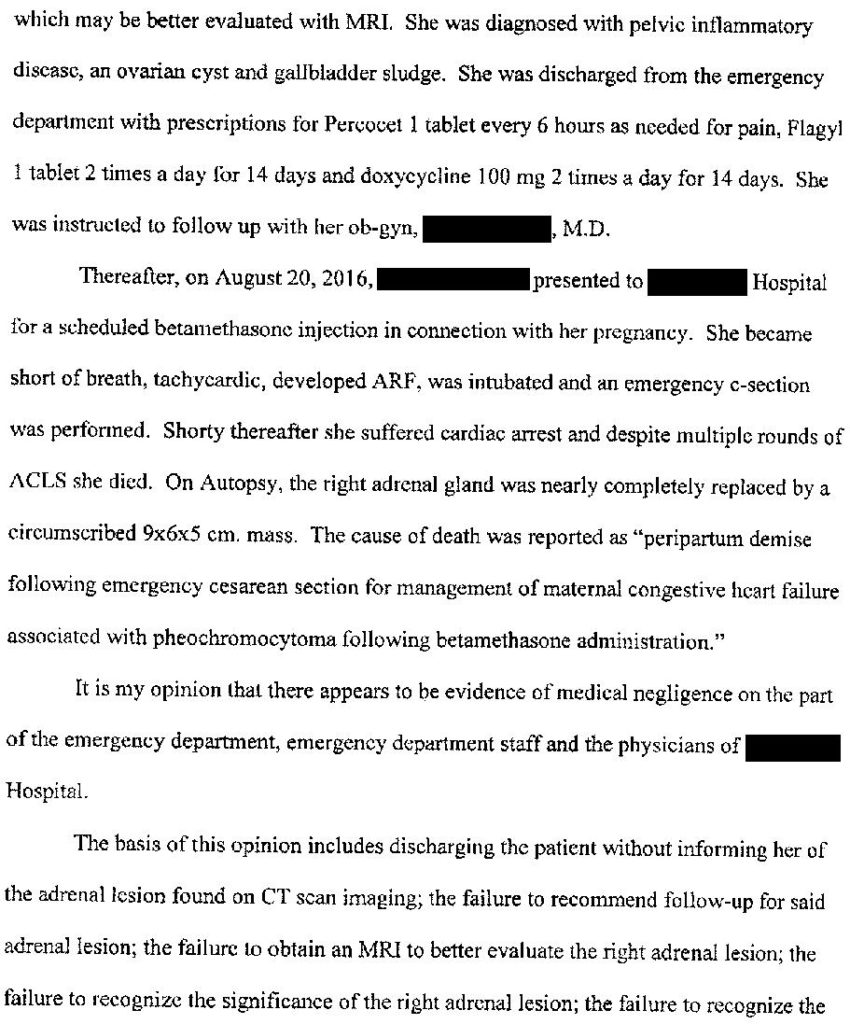
She was diagnosed with a UTI and PID, and started on Flagyl, doxycycline, and Macrobid.
Her symptoms resolved over the next few days.
6 months later in March 2016, she presented to her OBGYN after a positive pregnancy test.
Her prenatal care continued through August 2016.
She was diagnosed with cervical shortening at 31 weeks gestation.
Betamethasone was ordered (two 12mg injections, 24 hours apart).
The first injection was uneventful.
She returned the next day for the second injection.
She had become very short of breath in the past 24 hours.
Vitals included a HR of 160bpm and an O2 sat in the low 80s on room air.
The baby showed signs of severe fetal distress.
She was taken for an emergent C-section.
Shortly after delivery, the mother went into cardiac arrest.
Despite prolonged and aggressive attempts at resuscitation, she died.
The newborn girl survived 24 hours and also died.
An autopsy was done.
It revealed a 9 x 6 x 5 cm right adrenal mass, consistent with pheochromocytoma.
“Peripartum demise following emergency cesarean section for management of maternal congestive heart failure associated with pheochromocytoma and following betamethasone administration for fetal risk reduction due to maternal cervical insufficiency after surgical treatment of dysplasia”
The patient’s grief-stricken husband and family contacted an attorney.
A lawsuit was filed against the ER doctor, multiple OBGYNs who saw her, the NP at the OB clinic, and the hospital where this occurred.
The EM expert witness opinion is shown below:
An OBGYN expert was also hired:
The lawsuit was filed in 2018 is ongoing.
There have been no formal settlement offers.
I will update subscribers by email when there is a verdict.
Join the email list for updates and to get new cases when they’re published!
Pheochromocytomas are difficult to diagnose. They often present with vague symptoms that seem to randomly wax and wane with catecholamine surges. They are known as Great Imitators (along with multiple other diseases, covered in this fascinating Wikipedia article).
Pheochromocytoma crisis occurs when intense and prolonged catecholamine production results in end-organ damage. Surgery is a common trigger, but exogenous steroid administration can induce catecholamine production and sensitize target organs (as in this case). Stroke and MI are common manifestations, and often times the pheo crisis goes unrecognized. The challenge of making this diagnosis is reflected in the fact that about 50% are not diagnosed until autopsy (as in this case).
With the luxury of time and specialist consult, diagnosis is often made with plasma or urine metanephrine testing. These are usually send-out tests that will take weeks. During a crisis, severe hypertension and the presence of a large adrenal mass on CT are often the most recognizable clues.
Treatment of pheochromocytoma crisis usually involves use of alpha blockade, most commonly with phentolamine starting at a dose of 1mg/min.
This lawsuit highlights 2 key issues I’ve noticed over the years:
The deceased patient was a nurse. Patients who are healthcare workers or who have close family members who work in healthcare are much more likely to sue. I have no evidence to support this but it’s a theme I’ve noticed numerous times.
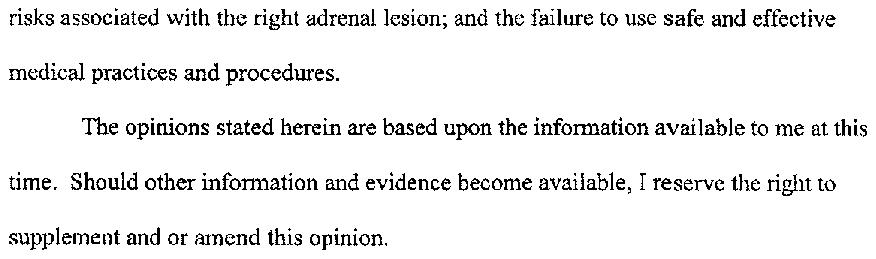
The failure to communicate or follow-up on incidental findings is one of the most common sources of malpractice lawsuits. We all have trained for years to make nuanced medical decisions and perform complicated procedures, only to fail the extremely basic step of communicating with patients about their finding and giving appropriate follow-up.
All of my research and sources are from these 2 excellent articles. If you’re like me and love to take a deep dive on these cases, I highly recommend you read them.