Hemorrhagic Shock Until Otherwise Proven
There are approximately 3.9 million annual visits for motor vehicle accidents to emergency departments,1 and a significant amount of emergency medicine residency addresses the care of trauma patients.
Hypotension after trauma should be treated as hemorrhage until proven otherwise. A recent change to 10th edition of ATLS guidelines in 2018 emphasized this, recommending only 1 liter of IV fluids before transfusing blood products instead of 1-2 liters of IV fluids recommended in the 9th edition of ATLS. This patient encounter occurred during the era of the 9th edition of ATLS. Per these dated ATLS recommendations, it was appropriate to give 2L IVF and vasopressors before the administration of blood. However, the patient was intermittently hypotensive and/or tachycardic for over 1.5 hours before receiving blood products.
Working in a resource-limited environment makes it very difficult to make judgments on the delay of administration of blood products without knowing the limitations and systems-based delays in ordering blood at this community hospital. We know from the defense expert witness deposition that the hospital where Dr. B worked at did not meet criteria for a Level I, II, or III trauma center. Both Dr. B (EM) and Dr. R (general surgeon) had allowed their ATLS certification to expire. (MedMalReviewer notes that requiring merit badges such as ATLS and ACLS are unnecessary for any physician who stays well-informed on modern emergency care).
This trauma patient was hypotensive prior to arrival in the ED, and blood wasn’t ordered until over 30 minutes after the patient arrived in the emergency department. It’s possible that the physician verbally ordered blood and/or had discussed with the blood bank prior to the 30 minute mark, however this was not mentioned in the MDM by the doctor or in the available nursing notes.
A Shock Index is a calculation that emergency physicians recognize inherently, but is a value that might be useful to formally recognize. It is calculated by dividing the heart rate by the systolic blood pressure, with normal ratios being 0.5-0.7. Studies have shown that a higher shock index is correlated with higher likelihood of requiring blood products and also higher mortality.2,3,4 While we don’t have exact documentation as to the titration of the pressors throughout this time, this patient had a shock index of >1.0 prior to arrival at the hospital that worsened throughout stay despite the use of IV fluids, vasopressors, and blood products.
| Time | Systolic BP | Heart Rate | Shock Index |
| EMS | 74 | 97 | 1.3 |
| EMS | 112 | 109 | 1.0 |
| 12:45 | 77 | 85 | 1.1 |
| 13:03 | 102 | 134 | 1.3 |
| 13:20 | 71 | N/A | —– |
| 14:03 | 67 | 117 | 1.7 |
| 14:06 | 103 | N/A | —– |
| 14:22 | 92 | 136 | 1.5 |
| 14:27 | 87 | 133 | 1.5 |
| 14:38 | 111 | 133 | 1.2 |
| 14:50 | 116 | 126 | 1.1 |
| 15:06 | 89 | 126 | 1.4 |
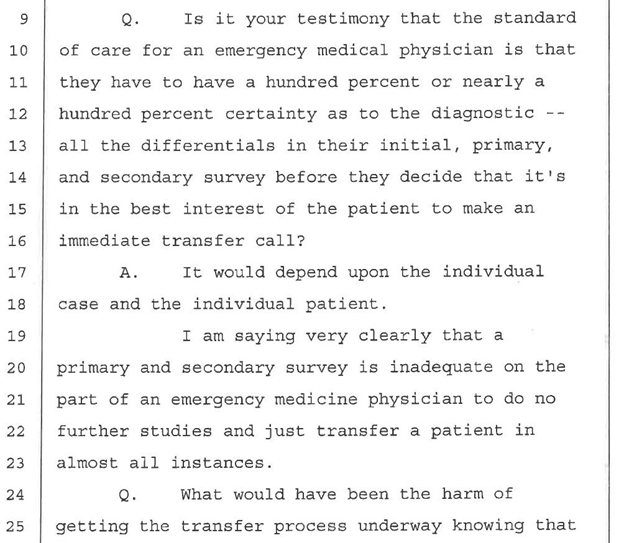
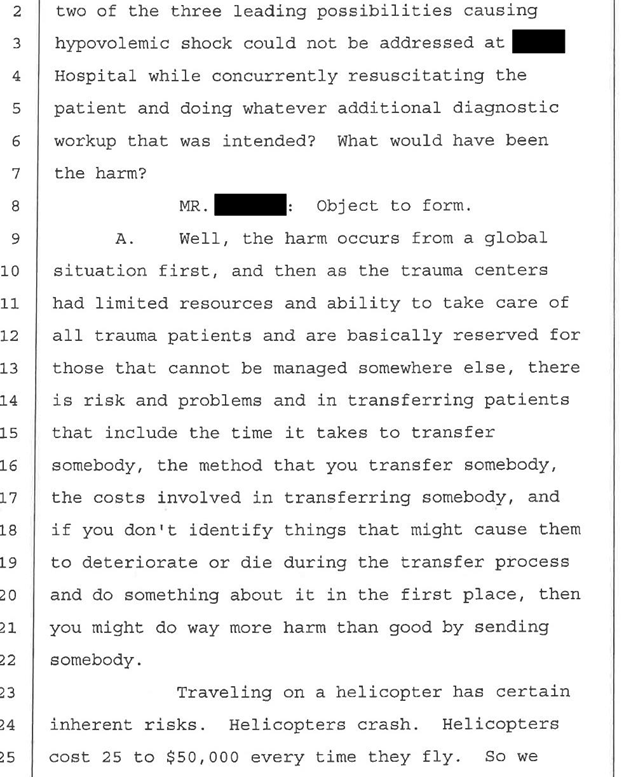
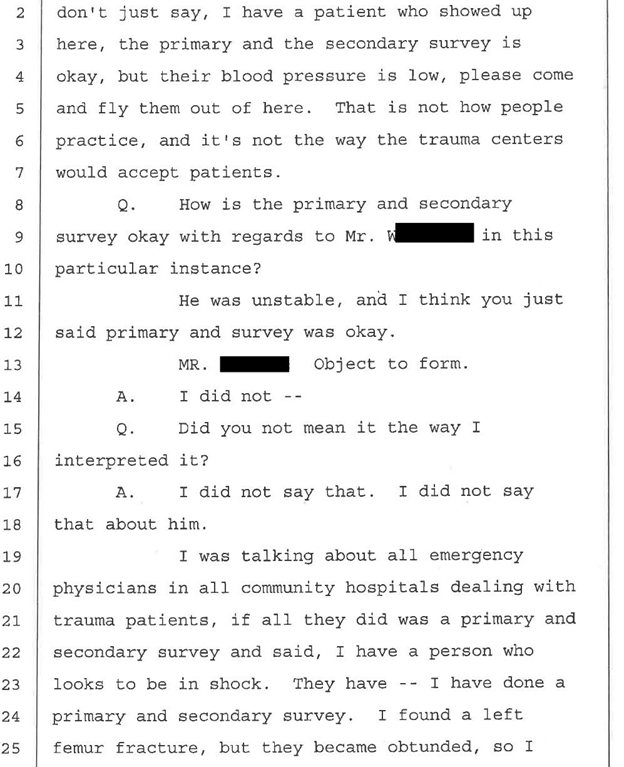
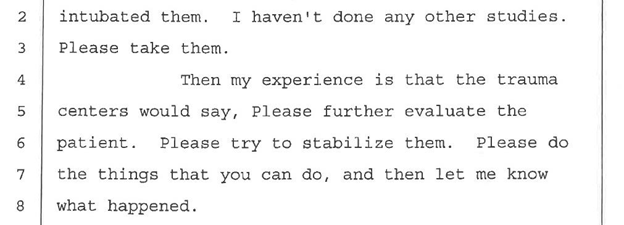
When to Transport
Transport for the patient was called just over two hours after the patient was in the emergency department, after the patient had returned from CT scan. About 30 minutes later, the helicopter arrived. Another focal point of the plaintiff complaint was the timeliness of the transfer to a tertiary care center. In the deposition of the emergency medicine physician defense expert witness, they discuss the problem with calling for transport early:
Consultant Notes and Shared Liability
The plaintiff expert witness disclosure notes that there was never a consult note left by the surgeon Dr. R, even though it is documented that the patient was at the bedside. Dr. B did a good job detailing his discussion with Dr. R, including their shared decision regarding disposition after the results of the panscan. Fortunately for Dr. R, he was later dismissed from the case.
Insist on notes from your consultants, especially in cases with an unfortunate outcome.
According to a review of consultant liability, “Determination of liability in the courts will rest, in part, on whether a physician-patient relationship was formed via an ‘affirmative act’. Consulting physicians may establish a relationship through an overt or implied agreement to participate in a patient’s care, or by reviewing specific tests and studies for the purpose of diagnosis and treatment.”5 Case law has established that in certain circumstances, a consultant may establish a physician-patient relationship by reviewing data for the purposes of planned treatment, even if they have never physically seen the patient.5
In Diggs v Arizona Cardiologists, Ltd., an emergency physician “curbsided” a cardiologist who was in the emergency department for another patient. The cardiologist, who reviewed the results, EKG, and history, and the emergency physician disagreed with the computer interpretation of MI, and discharged the patient with pericarditis. The cardiologist never saw the patient. The patient died of cardiac arrest from MI. Even though the cardiologist argued his consult was informal, “The court opined that the duty of care goes to the doctor most capable of preventing possible harm due to others’ negligence. [The cardiologist] was thus determined to be the most qualified to make treatment decisions in this case.”5
An excerpt from Moore et al. (2014) in ‘Shared Liability? Consultants, Pharmacists, and the Emergency Physician: Legal Cases and Caveats’:5
Continue to the next page to see the documentation review!
References:
- Albert M, McCaig LF. Emergency department visits for motor vehicle traffic injuries: United States, 2010–2011. NCHS data brief, no 185. Hyattsville, MD: National Center for Health Statistics. 2015.
- Cannon CM, Braxton CC, Kling-Smith M, Mahnken JD, Carlton E, Moncure M. Utility of the shock index in predicting mortality in traumatically injured patients. J Trauma. 2009;67(6):1426-1430. doi:10.1097/TA.0b013e3181bbf728
- Mutschler, M., Nienaber, U., Münzberg, M. et al. The Shock Index revisited – a fast guide to transfusion requirement? A retrospective analysis on 21,853 patients derived from the TraumaRegister DGU®. Crit Care 17, R172 (2013). https://doi.org/10.1186/cc12851
- Vandromme MJ, Griffin RL, Kerby JD, McGwin G Jr, Rue LW 3rd, Weinberg JA. Identifying risk for massive transfusion in the relatively normotensive patient: utility of the prehospital shock index. J Trauma. 2011;70(2):384-390. doi:10.1097/TA.0b013e3182095a0a
- Moore JJ, Matlock AG. Shared Liability? Consultants, Pharmacists, and the Emergency Physician: Legal Cases and Caveats. J Emerg Med 2014;46(5):612-616.
- Policy Statement: Emergency Medical Services Interfaces with Health Care Systems. February 2018. American College of Emergency Physicians.