The physician ordered a CBC, CMP, coagulation panel, and a CT scan of her head.
As expected, her INR was elevated at 2.4.

The CBC and CMP did not show any acute abnormalities. Copies of her full labs were not included in court documents.
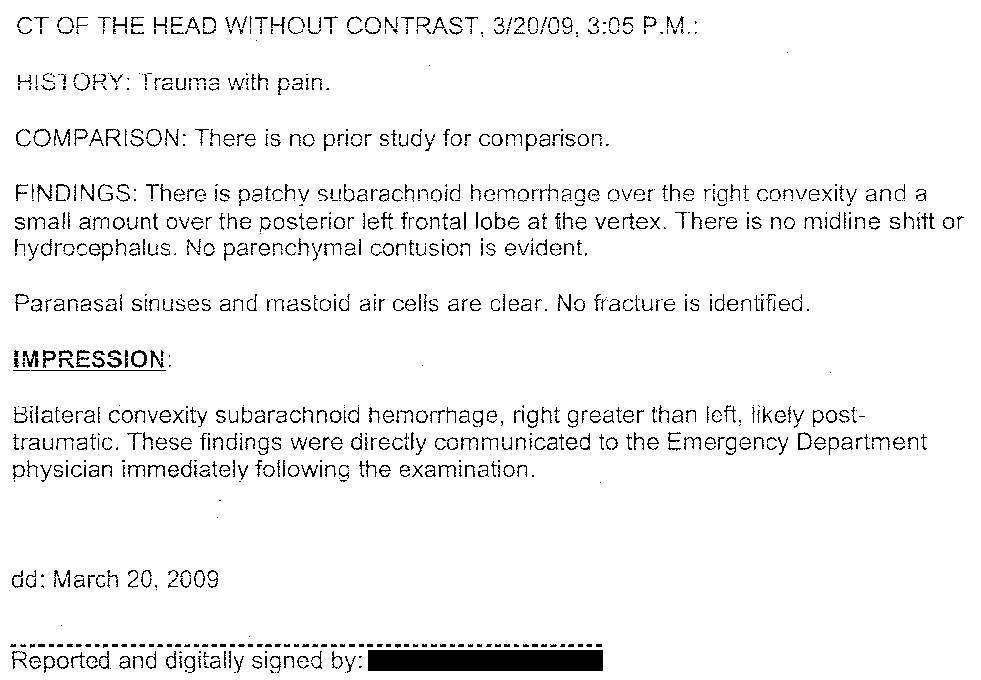
The results of the CT scan showed a subdural hematoma. The radiology report is shown below for email subscribers.
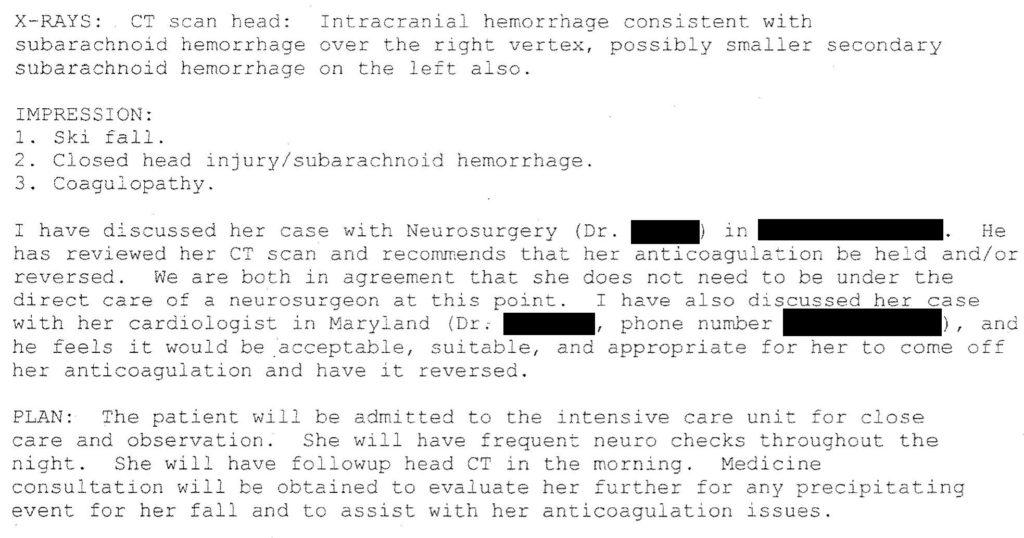
This hospital did not have a neurosurgeon. Therefore the general surgeon consulted the neurosurgeon at a nearby hospital.
At that time she had a GCS of 15 and no motor or sensory deficits. Therefore, both the neurosurgeon and general surgeon felt it was appropriate to defer transfer and watch her overnight.
The remainder of the general surgeon’s note is shown below.
The timeline of her ED care was relatively rapid. She arrived at 2:30pm, and by 3:05pm she had already had the CT scan of her head.
She was given a small dose of Ativan for anxiolysis in the CT scanner, and then given a dose of vitamin K after the bleed was identified.
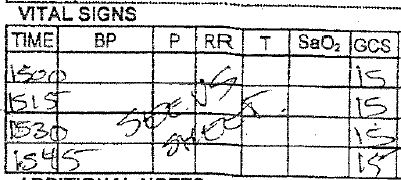
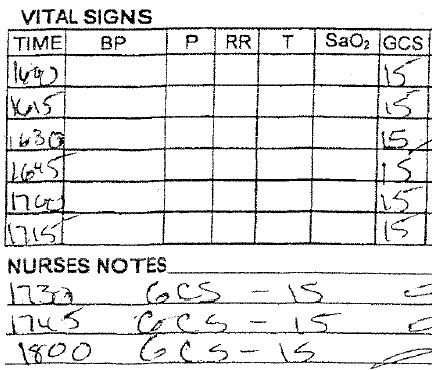
The ED nurses documented assessments of her GCS every 15 minutes. Her GCS was stable at 15 throughout her time in the ED.
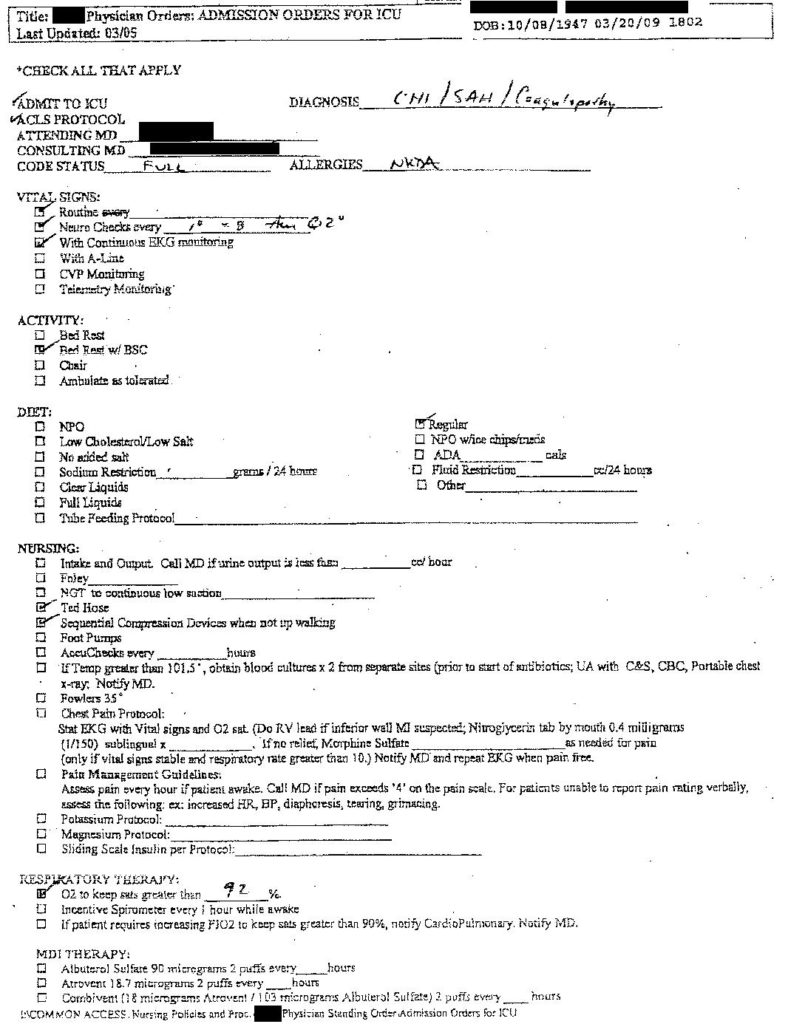
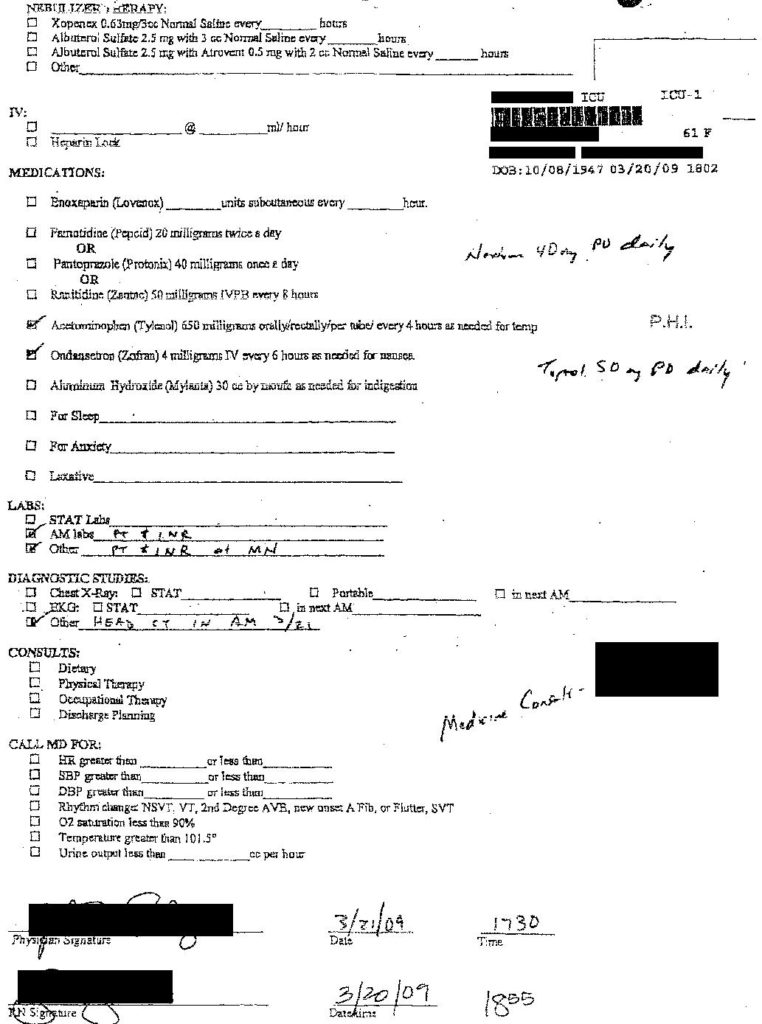
The general surgeon was the only doctor in the hospital. A hospitalist was consulted and technically assumed care of the patient, but the surgeon was responsible for writing admission orders and responding to any urgent inpatient needs.
The ICU admission orders are shown here:
What do you think the outcome in the ICU will be?
Continue to the next page to find out.